
II. Pathophysiology
- Epstein-Barr Virus
- Human Herpes Virus (Herpesviridae)
- Infects B Cells (B-Cell Lymphotrophic)
- Of those infected with EBV, 26-74% will not manifest Infectious Mononucleosis
- Transmission
- Transmission through infected Saliva (e.g. kissing, sharing drinks)
- Oral secretions transmit for up to 6 months
- May also be transmitted via genital secretions and sexual intercourse
- Incubation
- Range: 4-8 weeks (may be as short as 2 weeks)
- Life long infection
- Adults (by age 35 years) who have been previously infected and are carriers: 90-95% worldwide
III. Epidemiology
- No seasonal pattern
- No gender predisposition
- Adolescents and young adults
- Commonly occurs in congested, confined spaces
- College Students
- Military recruits (>0.9% annual Incidence)
IV. Symptoms
- Asymptomatic in 90% of cases
- Initial prodrome
- Mild-flu like symptoms for 3-5 days
- Classic symptom triad
- Fever (in >97% of cases)
- Persists for 7-10 days
- Severe Sore Throat
- Prominent Cervical Lymphadenopathy
- Large unilateral Anterior Cervical Lymphadenopathy is common
- However, Posterior Cervical Lymphadenopathy is more specific for Mononucleosis (LR+ 3.2)
- Fever (in >97% of cases)
- Other common symptoms
- Less common symptoms
V. Signs
- Common findings
- Exudative Pharyngitis or exudative Tonsillitis (>97%)
- Pharyngeal erythema and edema (85%)
- Prominent Cervical Lymphadenopathy (>97%)
- Posterior Cervical Lymphadenopathy (+LR 12) most common
- Axillary (+LR 21) and inguinal (+LR 2.9) Lymphadenopathy also common
- Other findings
- Splenomegaly (50 to 75%)
- Physical exam is unreliable in detecting Splenomegaly (which occurs in most patients with Mononucleosis)
- Present from as early as day 4 of illness (typically day 14) to as late as 8 weeks after onset
- Palatal Petechiae (50%, +LR 5.8)
- Periorbital edema (33%)
- Hepatomegaly (20%)
- Jaundice (8% of young adults, 26% of those over age 60 years old)
- Splenomegaly (50 to 75%)
VI. Labs
-
Streptococcal Rapid Antigen Test with reflex to Throat Culture
- Exclude coexisting Streptococcal Pharyngitis
- Concurrent Streptococcal PharyngitisIncidence: 4-30%
- If positive, avoid Amoxicillin due to rash
-
Complete Blood Count with differential
- Absolute Lymphocyte Count >4000 mm3
- Absolute Lymphocyte Count <4000 makes the Mononucleosis diagnosis unlikely
- Lymphocyte predominance: >50% of total White Blood Cell Count
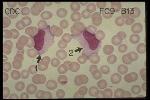
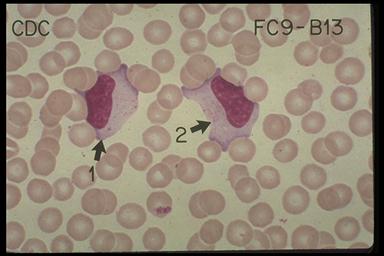
- Lymphocyte atypia >10%
- Very specific to EBV
- No further tests needed if Lymphocyte atypia present
- Efficacy: Combination of >50% Lymphocytes and >10% Atypical lymphocytes
- Test Sensitivity: 75%
- Test Specificity: 92%
- Other findings (see complications below)
- Hemolytic Anemia
- Mild Thrombocytopenia
- Platelet Count 100,000 to 150,000/mm3
- Neutropenia
- Neutrophil Count <1000/mm3
- Absolute Lymphocyte Count >4000 mm3
-
Liver Function Tests
- Increased liver transaminases in 80% of Mononucleosis cases
-
Heterophil Antibody Test (Monospot Test)
- Decreased Test Sensitivity in age <12 years old (esp. age <5 years) and in early infection (<1 week)
- False Positive tests do occur related to alternative diagnoses (see Monospot Test)
- Remains positive for up to one year after initial EBV infection
-
Epstein-Barr Virus Antibody
- Expensive and typically a send-out lab
- Consider in cases of high suspicion, negative Monospot test and results would change management
- Where VCA is Viral Capsid Antigen, EBNA is EBV-Associated nuclear Antigen (Test Sensitivity 97%, Specificity 94%)
VII. Differential Diagnosis
VIII. Diagnosis
IX. Management
- Symptomatic
- See Pharyngitis Symptomatic Treatment
- Relative rest (Pace activity for the day)
- Non-caffeinated fluids for adequate hydration
- Analgesics (NSAIDs or Acetaminophen)
- Avoid Aspirin
- Risk of Reye Syndrome
- Risk of worsening Thrombocytopenia
- Increased risk of Splenic Rupture
- Avoid strenuous Exercise or Contact Sport
- Risk of Splenic Rupture
- Return to play guidelines
- Return to play should be gradual
- Avoid splenic Ultrasound as a prognostic indicator for early return
- Three weeks: Moderate training allowed
- No Splenomegaly (not palpable or painful)
- No fever
- Liver Function Tests Normal
- Asymptomatic
- Four weeks: strenuous activity allowed
- Contact Sport participation may resume (if Splenomegaly has resolved)
- Severe odynophagia or Airway compromise
- Oral Prednisone 30-50 mg orally daily tapered over 10-14 days or
- Dexamethasone 0.3 mg/kg (up to 10 mg IV or oral)
- May require repeat doseing
- Antibiotics
- Only indicated for coexisting Streptococcal Pharyngitis (4% of cases)
- Maculopapular rash develops in 90% of EBV patients on antibiotics (esp. with Amoxicillin)
- Other ineffective agents
- No benefit with Acyclovir
- No benefit with Ranitidine
X. Complications: Most common
-
Splenic Rupture
- Spontaneous rupture in >50-80% of cases (remainder are Traumatic)
- Occurs in 0.5 to 1% of cases
- Mortality up to 9%
- Males account for 70% of rupture cases
- Timing: Days 4-21 from symptom onset (uncommon after 28 days, case reports up to 8 weeks)
- Diagnosis with CT Abdomen
- May present with Left upper quadrant pain (may radiate into left Shoulder)
- May present with significant hemodynamic instability including Hypotension, Syncope or Tachycardia
- Nonoperative management unless hemodynamically unstable
- Airway Obstruction
- Overall some sense of airway obstruction occurs in up to 25% of cases
- Significant airway obstruction occurs in 0.5 to 1% of cases (especially age <6 years old)
- Severe, life-threatening obstruction may occur with Stridor, Dyspnea, Tachypnea and Cyanosis
- Typically responds to Corticosteroids (see above)
- Rarely intervention may be needed (Endotracheal Intubation, Tracheostomy, Tonsillectomy)
XI. Complications: Other
- Cardiopulmonary
- Pneumonitis
- Pericarditis
- Viral Myocarditis
- May present with Chest Pain and ischemic EKG changes
- Neurologic complications (1-5% of cases)
- Encephalitis
- May present with Altered Level of Consciousness, combative behavior or Seizure
- Encephalitis complications may persist longterm in up to 40% of cases
- Viral Meningitis
- Guillain-Barre Syndrome
- Bell's Palsy
- Retrobulbar neuritis
- Syndrome of Inappropriate Antidiuretic Hormone (SIADH)
- Multiple Sclerosis (EBV postulated as one possible causative factor)
- Encephalitis
- Malignancy
- Lymphoproliferative Disease and malignant transformation risk factors
- HIV Infection
- Immunodeficiency (e.g. X-linked lymphoproliferative disease)
- Transplant recipients (mortality approaches 50%)
- Burkitt Lymphoma
- Nasopharyngeal Cancer
- Hodgkin Disease
- Lymphoproliferative Disease and malignant transformation risk factors
- Hematologic
- Hemolytic Anemia (3%)
- Hemophagocytic Lymphohistiocystosis
- Thrombocytopenia
- Presents between weeks 3 to 5 from symptom onset and resolves by week 6
- Mild Thrombocytopenia (Platelet Count 100-150k/mm3) in 25-50% of Mononucleosis cases
- Severe Thrombocytopenia (Platelet Count <20k/mm3) occurs rarely and resolves spontaneously
- Neutropenia (3%)
- Neutrophils <1000/mm3, may persist for up to 2 weeks
- Head and neck
- Peritonsillar Abscess (0.2%)
- Viral Sialoadenitis (especially Parotid Gland)
- Other
- Acute Interstitial Nephritis
- Severe Hepatitis
- Autoimmune Disorders (e.g. Systemic Lupus Erythematosus, Rheumatoid Arthritis)
- Fulminant Epstein Barr Virus Infection
- Immunocompromised state
- X-Linked Lymphoproliferative Syndrome (associated with a 96% mortality rate)
XII. Associated Conditions
- Streptococcal Pharyngitis carriage accompanies Mononucleosis in up to 30% of cases
- Chronic Fatigue Syndrome (possibly same viral agent)
XIII. Course
- Acute illness phase typically resolves within 1-2 weeks
- Athletes require 3-6 months to return to prior fitness
- Fatigue or Hypersomnia persists 6 months in 9-22%
-
Fatigue present
- Initial: 77%
- Month 1: 28%
- Month 2: 21%
- Month 6: 13%
-
Hypersomnia present
- Initial: 45%
- Month 1: 18%
- Month 2: 14%
- Month 6: 9%
-
Arthralgias present
- Initial: 23%
- Month 1: 15%
- Month 2: 6%
- Month 6: 9%
- References
XIV. Resources: Patient Education
- AAFP Family Doctor Patient Education Handout
XV. References
- Gantz in Noble (2001) Primary Care, p. 267-71
- Katz in Gershon (2004) Krugman's ID, p. 143-55
- Peoples (2014) Crit Dec in Emerg Med 28(3): 11-6
- Ebell (2004) Am Fam Physician 70(7):1279-87 [PubMed]
- Luzuriaga (2010) N Engl J Med 362(21):1993-2000 [PubMed]
- Sylvester (2023) Am Fam Physician 107(1): 71-8 [PubMed]
- Womack (2015) Am Fam Physician 91(6): 372-6 [PubMed]