
II. Epidemiology
III. Risk Factors
- HIV with CD4 Count related risk of Pneumocystis
-
Immunosuppression in non-HIV conditions
- Solid organ or Hematopoietic Stem Cell Transplant recipients
- High dose Corticosteroids (Prednisone 20 mg or higher)
- Cancer Chemotherapy patients
- Rheumatologic Disease
- References
IV. Pathophysiology
- Pneumocystis defies classification
- Both Protozoan and Fungal Characteristics
- Recently renamed as Pneumocystis jiroveci
- Ubiquitous organism
- Most humans and mammals exposed early in life
- Clinically Significant infection occurs in AIDS with CD4 Count <250 cell/ul
- Clinical infection may represent reactivation
V. Symptoms
- Symptoms usually develop over 1-2 weeks
- Typical Bacterial Pneumonia develops over 3-5 days
- Initial Symptoms (occur in 66%, often subtle)
- Pronounced Symptoms
- Sputum production
- Chest Pain
- Chills
- Exertional Dyspnea
- Profound Hypoxia occurs with even just a few steps taken
VI. Labs
-
White Blood Cell Count Normal
- Elevated WBC Count in typical Bacterial Pneumonia
-
Lactate Dehydrogenase (LDH) > 350 units/L associated with PCP
- Test Sensitivity: 78 to 100%
- Normal LDH may decrease the likelihood of PCP
- Test Specificity: 35 to 78%
- Elevated LDL also seen with Bacterial Pneumonia and Tuberculosis
- Test Sensitivity: 78 to 100%
-
Sputum induction
- Methods
- Efficacy
- Test Sensitivity 80-90% for Pneumocystis (induced Sputum with PCR)
- However expectorated Sputum has low Test Sensitivity
- Negative Predictive Value only 50-60%
- Test Sensitivity 80-90% for Pneumocystis (induced Sputum with PCR)
- Examination stains
- Methenamine silver
- Giemsa stains
- Serum Beta D-Glucan
- High False Positive Rate
- Negative Predictive Value >95%
- Efficacy in AIDS for Beta D-Glucan >80 pg/ml
- Test Sensitivity: 92%
- Test Specificity: 65% (75% if respiratory symptoms)
- References
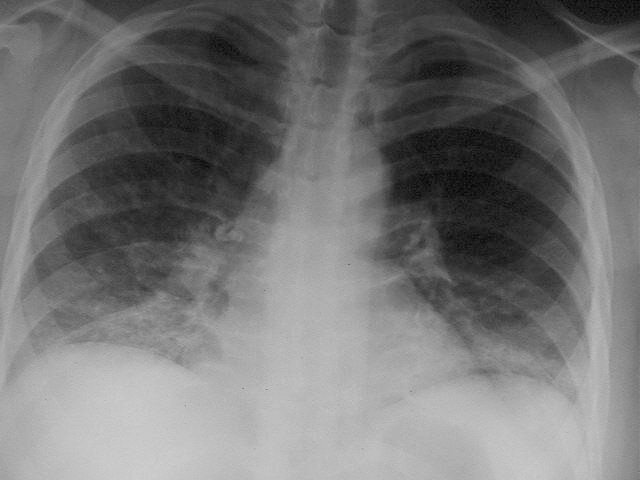
VII. Imaging: Chest XRay
- Diffuse bilateral Interstitial Infiltrates (80-95%)
- Seen in Tuberculosis
- Seen in Bacterial Pneumonia
- Bat winging appearance
- Focal infiltrates rarely seen with Pneumocystis
- Images

VIII. Diagnosis
- Clinical diagnosis
- Definitive diagnosis is typically by bronchoalveolar lavage
- Factors suggestive of PCP
- Interstitial Infiltrates AND Thrush (Odds Ratio 11.8)
- Exertional Dyspnea
- Inspiratory crackles
- Subacute disease course
IX. Management: General
- Treatment Duration for 21 days (followed by PCP Prophylaxis)
- Treatment protocols are based on level of illness (esp if PaO2 <70 mmHg)
- Initiate Antiretroviral therapy within 2 weeks of PCP diagnosis (HIV patients)
X. Management: First-line agents
- Duration: 21 days of treatment and then prophylaxis
- Not critically ill (PaO2 >70 mmHg) and able to take oral medications
- No Corticosteroids indicated
- Trimethoprim-Sulfamethoxazole (Bactrim, Septra) DS 2 tabs orally every 8 hours (15 mg/kg of trimethoprim/day)
- Adverse reactions occur in 40-60% within 3 weeks
- Alternative (Fewer dose limiting adverse reactions, but risk of Methemoglobinemia)
- Dapsone 100 mg orally every 24 hours AND Trimethoprim 5 mg/kg orally every 8 hours
- Critically ill with Hypoxia (PaO2 <70 mmHg or A-a Gradient >35) or unable to take oral medications
- Start Corticosteroids 15-30 min before antibiotics (see dosing below)
- Trimethoprim-Sulfamethoxazole (Bactrim, Septra) 15-20 mg/kg of trimethoprim/day IV divided every 6-8 hours
XI. Management: Alternative Regimen
- Duration: 21 days of treatment and then prophylaxis
- Not critically ill (PaO2 >70 mmHg) and able to take oral medications
- No Corticosteroids indicated
- Clindamycin 600 mg IV or 300-400 mg PO every 6 hours AND
- Primquine 15-30 mg of based every 24 hours or Atovaquone 750 mg po bid
- Critically ill (PaO2 <70 mmHg or A-a Gradient >35) or unable to take oral medications
- Start Corticosteroids 15-30 min before antibiotics (see dosing below)
- Clindamycin 600 mg IV every 8 hours AND Primquine 15-30 mg of based every 24 hours OR
- Pentamidine 4 mg/kg/day IV (or IM)
XII. Management: Corticosteroids
- Efficacy
- Prevents alveolar inflammation and exudation
- Results from the killing of Pneumocystis organisms
- Reduces the risk of intubation and death by 50%
- Indications (based on Arterial Blood Gas)
- Arterial pO2 < 70 mmHg
- A-a Gradient > 35 mmHg on room air
- Dosing: Prednisone
- Start: 40 mg twice daily for 5 days
- Next: 40 mg every 24 hours for 5 days
- Taper: 20 mg every 24 hours for 11 days
XIII. Prevention: Pneumocystis Prophylaxis
- Indications
- CD4 Count <200 cells
- HIV patients with respiratory symptoms
- Duration
- Continue prophylaxis until CD4 Count >200 for at least 3 months
- First-Line Protocol
- Alternative Protocols
- Pentamidine 300 mg in 6 ml sterile water aerosolized every 4 weeks OR
- Atovaquone 1500 mg orally every 24 hours with food OR
- Dapsone 200 mg and Pyrimethamine 75 mg AND Folinic Acid 25 mg once each week
XIV. Prognosis
- Treated appropriately: 10 to 20% mortality
- Higher mortality with severe infections
- Untreated: Uniformly fatal
XV. References
- Parker and Bond (2023) Crit Dec Emerg Med 37(10): 4-9
- Gilbert (2017) Sanford Guide (accessed IOS version 8/3/2017)
- Weller (2001) BMJ 322:1350-4 [PubMed]