
II. Indications
- Regional Anesthesia to allow for procedures (in place of Procedural Sedation)
- Severe localized pain control (e.g. Femur Fracture)
III. Contraindications
-
Anticoagulation is NOT a contraindication to Nerve Blocks
- However, best to perform block at compressible site
- Infection overlying injection site
- Limb Compartment Syndrome suspected
- Allergy to medication components
- Serial Neurologic Exam required
- Patient unable to report pain or Paresthesias at injection site (suggests nerve injection)
- Altered Mental Status or sedation
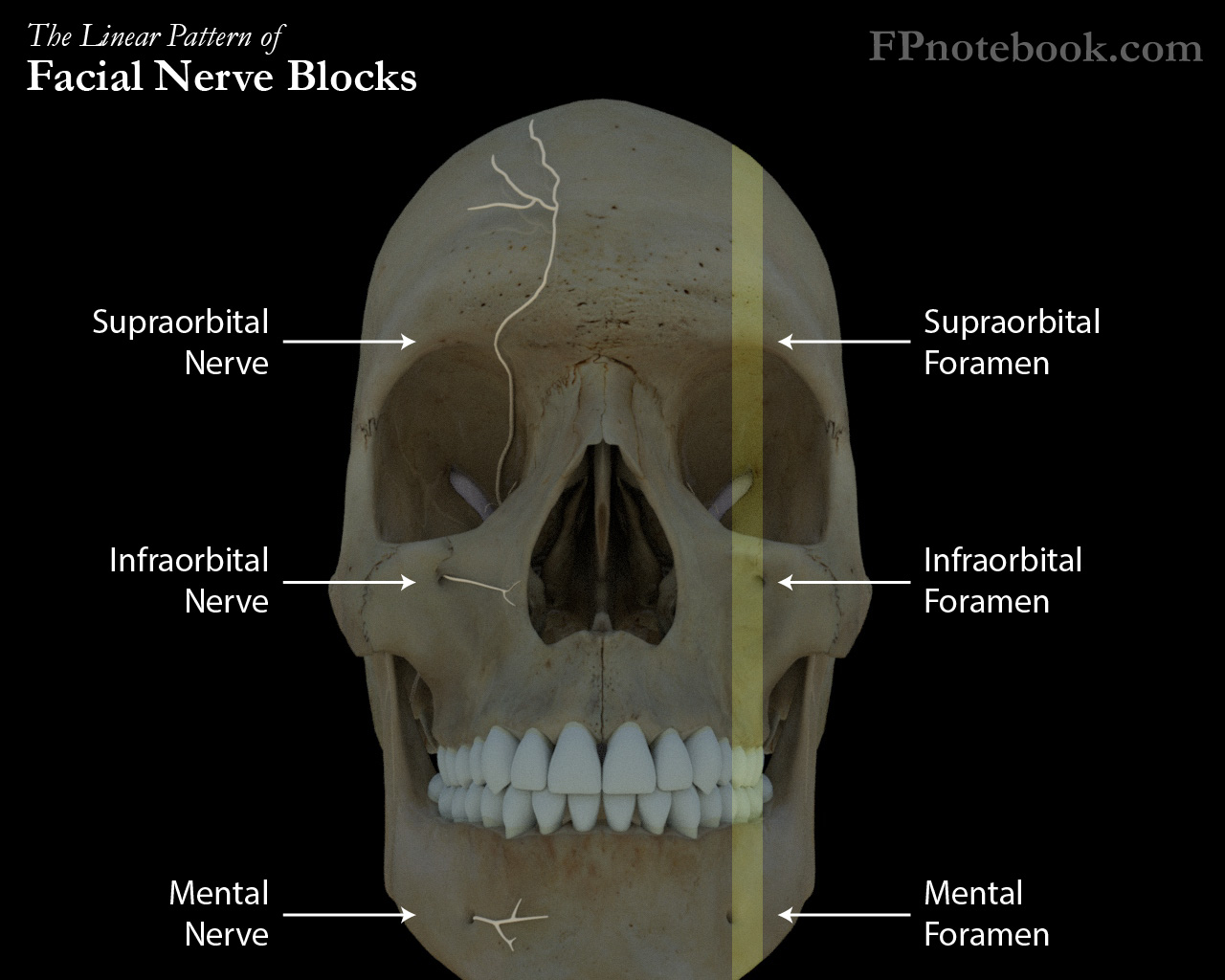
IV. Types: Head and Neck
- Images
- Occiput
- Ear
- Regional Anesthesia for the Forehead
- Regional Anesthesia for the Central Face
- Regional Anesthesia for the Anterior Mandible
- Lips
- Teeth
- Neck
V. Types: Trunk (Chest Wall including Ribs)
- Erector Spinae Plane Block
- Serratus Anterior Nerve Block
- Intercostal Nerve Block
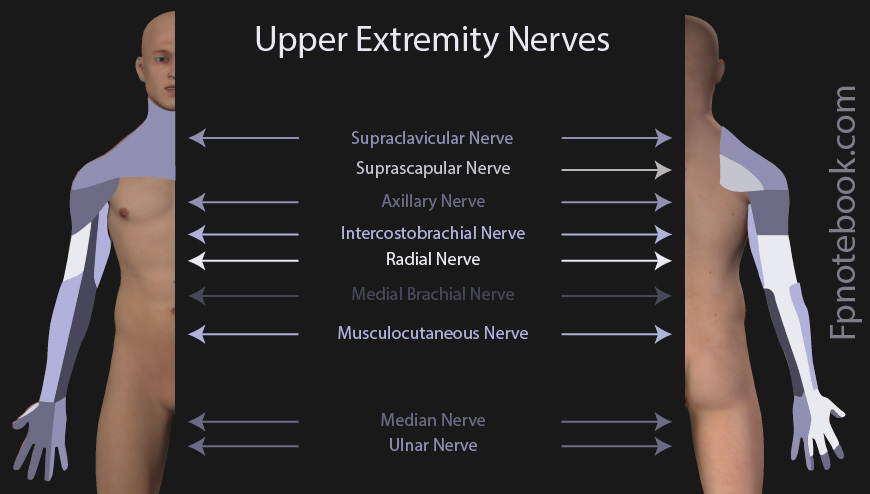
VI. Types: Arm
- Images
- Neck and upper chest
- Superficial Cervical Plexus Block (anterolateral neck and clavicle)
- Shoulder
- Upper arm and elbow
- Interscalene Brachial Plexus Block (includes Shoulder)
- Supraclavicular Brachial Plexus Block (entire arm distal to Shoulder)
-
Forearm and hand
- Infraclavicular Brachial Plexus Block (includes elbow)
- Axillary Brachial Plexus Block
- Elbow
- Wrist
VII. Types: Leg
- Images
- Hip
- Lower leg (below knee)
- Popliteal Sciatic Nerve Block (peroneal nerve and tibial nerve)
- Ankle

VIII. Complications
- Nerve injury with persistent Paresthesias
-
Local Anesthetic System Toxicity (LAST Reaction)
- Intravascular injection of Anesthetic results in Seizures, Arrhythmias or Cardiac Arrest
- Calculate toxic dose levels in advance of injection, and stay well below these levels
- Highest risk with Bupivacaine (lowest risk with Ropivacaine)
- Ropivacaine toxicity presents with neurologic findings
- Bupivacaine toxicity presents with Cardiac Arrhythmias
- Treated with Intralipid (20% IV fat emulsion) 1.5 ml/kg bolus, then 0.25 ml/kg/min until stable
- Airway management and treat Seizures with Benzodiazepines
IX. Exam
- Identify region of Anesthesia needed (and most appropriate Nerve Block to adequately cover that region)
- Focused Peripheral Nerve exam
X. Preparation: General
- Informed Consent
-
Intravenous Access and Intralipid available
- See LAST Syndrome under complications
- Have a low threshold in giving Intralipid early when suspected LAST Reaction
-
Ultrasound
- High frequency linear probe is preferred
- Exception: Deeper structures (e.g. hip) may require curvilinear probe
- Stand-off pad (or copious Ultrasound gel) may be needed in regions where Peripheral Nerve is superficial
- Pre-scan with Ultrasound and identify needle insertion site
- Nerve will appear as starry night within annular structure (or honey comb)
- Nerves exhibit anisotropy, and simply tilting probe slightly can help discriminate nerve tissue
- Consider marking the insertion site and landmarks
- Ultrasound significantly lowers complication rate (nerve injury, intravascular injection)
- Superficial Nerve Blocks are considered clean procedures (similar to IV Access)
- These are typically performed with an antiseptic cleaned probe without probe cover
- See Skin Preparation below
-
Joint Injections and deep injections (e.g. hip) and catheter insertions should use full sterile technique
- Cover probe with sterile Ultrasound probe cover (or transparent dressing such as Tegaderm)
- Drape surrounding skin
- High frequency linear probe is preferred
-
Skin Preparation
- Apply Topical Antiseptic to region of needle insertion site
- Chlorhexidine (Hibiclens, preferred)
- Povidone-Iodine (Betadine)
- Apply Topical Antiseptic to region of needle insertion site
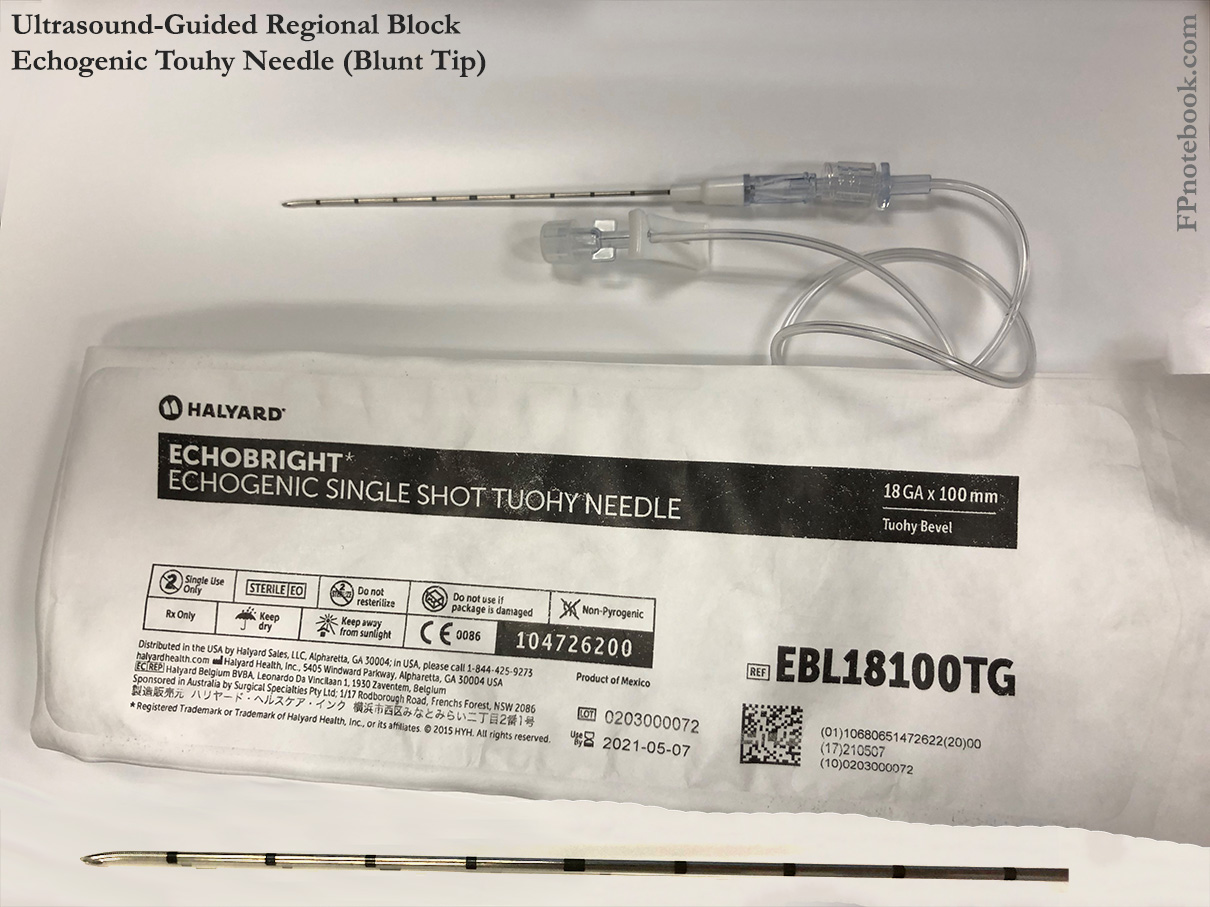
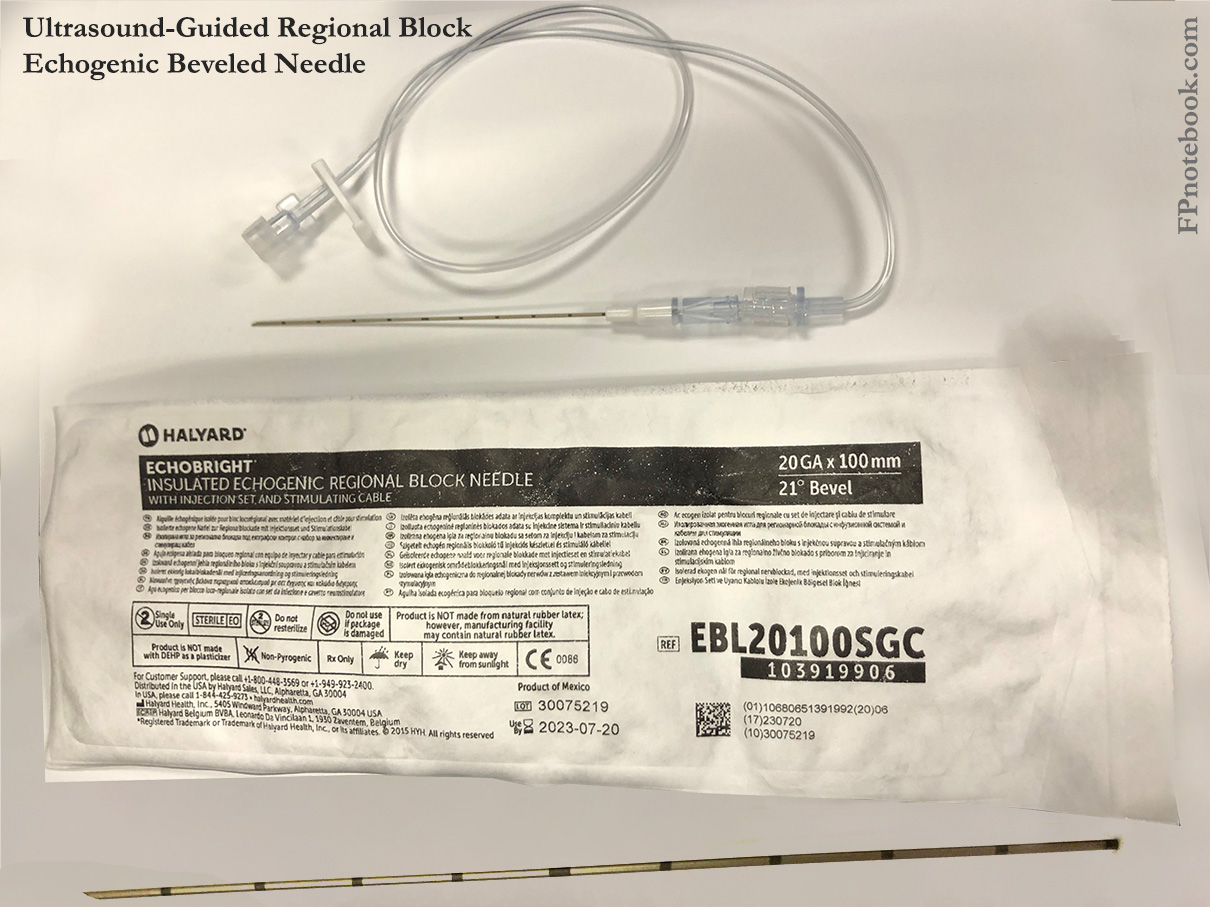
- Needles
- Images
- Blunt tip needles or Tuohy Needles (preferred over cutting needles)
- Blunt tip needles allow for better tactile feedback at fascial planes and less risk of nerve injury
- Needle sizes
- Gauge: 25 to 27 gauge (up to 18-22 gauge in some cases)
- Length: 1.5 inches (up to 3 inches in some cases)
- Images
- Maximum Dosing
- Use Ideal Body Weight
- Adjust doses for poor nutritional intake, Cachexia
- Avoid doses close to the maximum for drugs with significant LAST Reaction (e.g. Bupivacaine cardiotoxicity)
- Drugs such as Ropivacaine may be used more safely at doses close to maximum per Ideal Body Weight
- Avoid combining Anesthetics
- Maximum dose is unpredictable when combined with other agents (adverse effects are additive)
- Individual Anesthetic maximum doses are not reliable when agents are combined
-
Anesthetic Metabolism
- Metabolism is not typically Clinically Significant for single dose injection regional blocks
- However, continuous infusion regional blocks are significantly affected by metabolism
- Monitor hepatic function (e.g. INR) and Renal Function (e.g. eGFR) and adjust as needed
- Lidocaine undergoes renal metabolism
- Bupivacaine and Ropivacaine undergo hepatic metabolism
- Modifying Anesthetic duration
- Prolonged Anesthetic effect is often desired in very painful injuries (e.g. Rib Fractures, Hip Fractures)
- However, extremity blocks result in transient paralysis and risk of Pressure Injury from sensory deficit
- Use short acting Anesthetic (e.g. Lidocaine) when Regional Anesthesia is only needed for brief procedure
- Joint dislocation or extremity Fracture reduction are often ideal for short duration Anesthetic
- Additives that prolong Anesthetic activity (often both Dexamethasone and Epinephrine are both added to Anesthetic)
- Dexamethasone 4 mg/ml at typical dose of 4 mg or 1 ml (up to 10 mg or 2.5 ml)
- Epinephrine 1:200,000 final concentration (when combined with Anesthetic)
- Add 0.1 mg (1 ml of 1:10,000 Epinephrine) to every 20 ml of Local Anesthetic
- Prolonged Anesthetic effect is often desired in very painful injuries (e.g. Rib Fractures, Hip Fractures)
-
Anesthetic volume
- Volume is more important than concentration for block efficacy
- Blocks most commonly fail for lack of adequate volume
- Best to dilute Anesthetic to lower concentrations and higher volume (better efficacy, lower toxicity)
- Dilute with Normal Saline
- Based on Nerve Block type
- Plane blocks (e.g. Fascia Iliaca Block) fills a virtual plane between Muscle or fascial layers
- Requires larger volumes of Anesthetic (often 30 to 60 ml in adults)
- Peripheral Nerve Blocks
- Relatively smaller volumes of Anesthetic are used compared with plane blocks
- The injection is localized around the target nerve and Ultrasound demonstrates the proximity
- Plane blocks (e.g. Fascia Iliaca Block) fills a virtual plane between Muscle or fascial layers
- Volume is more important than concentration for block efficacy
- Other precautions
- Inject Anesthetic slowly to reduce pain
- Avoid adding bicarbonate to Ropivacaine and Bupivacaine (may crystallize solution)
- Inject deep to target nerves
- Avoids obscuring target nerve structures on Ultrasound if injection solution contains bubbles
XI. Preparation: Anesthetic Selection
-
Anesthetic: Amides (two i's in their names)
- Mepivacaine 1 to 1.5% (10 to 15 mg/ml)
- Maximum dose: 4 mg/kg
- Onset: 10-20 minutes
- Duration: 45 to 90 minutes up to 3 hours
- Lidocaine 1 to 2% (10 to 20 mg/ml)
- Maximum dose: 4 mg/kg
- Onset: 5-10 minutes
- Duration: 30 to 60 minutes (longer with Epinephrine)
- Bupivacaine (Marcaine, Sensorcaine) 0.25% or 0.5% (2.5 to 5 mg/ml)
- Onset: 5 minutes (up to 15-30 minutes)
- Duration: 2 to 4 hours (up to 6 hours, esp. when combined with Epinephrine)
- Max bolus dose: 2 mg/kg (some guidelines use maximum of 2.5 mg/kg)
- Weight >=75 kg (165 lb): 60 ml of 0.25% (2.5 mg/ml) or 30 ml of 0.5% (5 mg/ml)
- Avoid in pregnancy (increased Bioavailability, crosses placenta)
- Always confirm not intravascular (withdraw first) as risk of lethal Arrhythmias (Ventricular Fibrillation)
- See LAST Reaction
- Less risk of systemic absorption when combined with Epinephrine
- Ropivacaine 0.2 to 0.5% (2 to 5 mg/ml)
- Preferred agent in Regional Anesthesia (decreased LAST toxicity risk)
- Decrease dose in liver disease, malnourishment, Critical Illness
- Single bolus
- Onset: 10-20 minutes
- Duration: 6 to 14 hours
- Maximum Dose: 3 mg/kg of 0.5 % (5 mg/ml)
- Weight 50 kg (110 lb): Maximum 30 ml of 0.5% (1 bottle of Ropivacaine)
- Weight 60 kg (132 lb): Maximum 36 ml of 0.5%
- Weight 70 kg (154 lb): Maximum 42 ml of 0.5%
- Weight 80 kg (176 lb): Maximum 45-48 ml of 0.5%
- Weight 90 kg (198 lb): Maximum 45-54 ml of 0.5%
- Weight >=100 kg (220 lb): Maximum 45-60 ml of 0.5% (up to 2 bottles of Ropivacaine)
- Continuous infusion
- Maximum: 0.5 mg/kg/h of 0.2% (2 mg/ml)
- Weight 40 kg: Maximum 10 ml/h of 0.2% (2 mg/ml)
- Weight 50 kg: Maximum 12 ml/h of 0.2% (2 mg/ml)
- Weight >=56 kg: Maximum 14 ml/h of 0.2% (2 mg/ml)
- Maximum: 0.5 mg/kg/h of 0.2% (2 mg/ml)
- References
- Reardon and Martel (2020) Regional Anesthesia for Acute Care Conference, attended 12/11/2020
- Mepivacaine 1 to 1.5% (10 to 15 mg/ml)
-
Anesthetic: Esters (Indicated in amide Anesthetic allergy)
- Pontocaine 0.25% (2.5 mg/ml)
- Maximum dose: 1.5 mg/kg
- Onset: 15-30 minutes
- Duration: 2 to 3 hours
- Chloroprocaine 1-2% (10 to 20 mg/ml)
- Maximum dose: 6 mg/kg
- Onset: 15-30 minutes
- Duration: 30 to 60 minutes
- Pontocaine 0.25% (2.5 mg/ml)
-
Diphenhydramine (Benadryl)
- Diphenhydramine may be used as an alternative regional Anesthetic in allergy to esters and amides
- Diphenhydramine duration: 6 to 10 hours of regional Anesthetic effect
- Use the IV Solution injected regionally
XII. Technique: Ultrasound-Guided Block
- Background
- Ultrasound guided Nerve Blocks are preferred over external landmarks and Peripheral Nerve stimulation guidance
- Ultrasound reduces failed Nerve Block, neurovascular injury and shortens procedure time
-
Ultrasound probe
- High Frequency linear probe (5 to 12 MHz) is used for most Nerve Blocks
- Prepped with sterile cover as above
- Held in non-dominant hand
- Some needles may be magnetized for better visualization on Ultrasound
- Needle is best visualized when perpendicular to Ultrasound probe (e.g. extremity blocks)
- Ultrasound probe beam angle settings may be adjusted/angled to remain perpendicular to needle
- Allows for better needle visualization
- In-Plane Approach (preferred if anatomy allows)
- Almost always used in Regional Anesthesia (instead of out-of-plane)
- Needle enters on one side of probe long-axis (parallel to the probe)
- Needle may be followed along its entire length
- Requires fine control of probe and needle due to narrow width of the Ultrasound beam (3 mm)
- Fan the probe slightly from side to side to visualize the needle
- Out-Of-Plane Approach
- Needle enters at center of probe (perpendicular to the probe)
- Requires probe to fan with the needle insertion to follow the distal needle tip
- Absolute needle tip may be difficult to distinguish from other positions on the needle shaft
- Needle insertion
- Gradually advance needle, making slight angle adjustments as approaching target
- Advance needle until adjacent but not within the nerve
- Slightly withdraw needle if Paresthesias or pain is experienced
-
Anesthetic injection
- Withdraw first to confirm that needle is not intravascular
- First inject a small volume of Anesthetic adjacent to nerve (visualize on Ultrasound)
- Some providers use Normal Saline for initial identification of needle position
- Observe for Anesthetic spread on Ultrasound (tissues separate)
- Lack of Anesthetic spread may indicate intravascular injection
- Withdraw needle if Paresthesia or pain occurs
- Wait to inject at new location until symptoms resolve
- Inject at several sites around the nerve
- Results in encasing the nerve in a wide ring of fluid
- Evaluation of Nerve Block efficacy
- Test the region of Nerve Block over the subsequent 10-15 minutes
- Wait to initiate procedure until adequate Anesthesia achieved
XIII. Resources
- Local Anesthetics: Clinical Pharmacology and Rational Selection
- Upper Extremity Nerve Blocks (AAFP, Includes diagrams and videos)
XIV. References
- Eicken and Rempell (2016) Crit Dec Emerg Med 30(4):3-11
- Reardon and Martel (2020) Regional Anesthesia for Acute Care Conference, attended 12/11/2020
- Swaminathan and Stone in Herbert (2019) EM:Rap 19(3): 3-4
- Yurgil (2020) Am Fam Physician 101(11):654-64 [PubMed]