
II. Pathophysiology
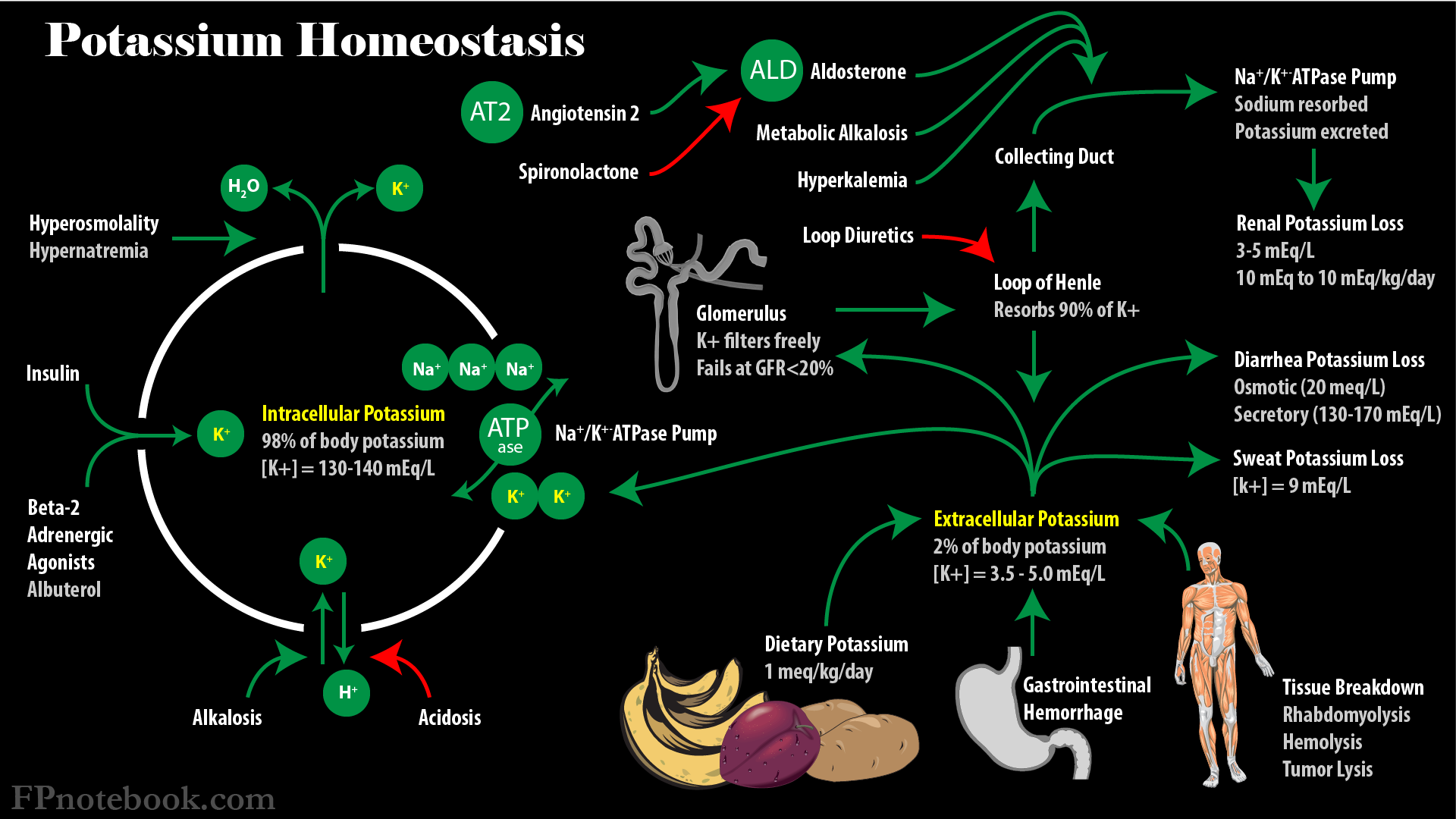
- See Potassium Homeostasis
- Images
III. Epidemiology
-
Prevalence
- General population: 3.3%
- Emergency Department: 3.6%
- Chronic Kidney Disease: 18%
- Inpatient: 6.9 to 12.3%
- Brookes (2021) Intern Med J 51(11): 1906-18 [PubMed]
- Kovesdy (2018) Eur Heart J 39(17): 1535-42 [PubMed]
- Singer (2017) Clin Exp Emerg Med 4(2): 73-9 [PubMed]
IV. Causes
V. Findings: Signs and Symptoms
- Symptoms occur when Serum Potassium > 6.0 to 6.5 meq/L
- Neurologic Changes
- Weakness
- Paresthesias
- Areflexia
- Ascending paralysis
- Respiratory Failure
- Cardiovascular Changes
- Bradycardia to Asystole or Ventricular Fibrillation
- AV prolonged transmission to complete Heart Block
VI. Labs
- Chemistry Panel
- Serum Potassium
- Serum Electrolytes including serum bicarbonate
- Renal Function tests (BUN, Creatinine)
- Spot urine for Urine Potassium, Urine Sodium and Urine Creatinine
- Fractional Excretion of Potassium
- Transtubular Potassium Gradient
- Urine Sodium <25 mEq/L suggests decreased distal renal flow
- Other labs to consider (see evaluation below)
- Serum Aldosterone
- Serum renin
VII. Diagnostics: Electrocardiogram
-
General
- EKG changes occur when Serum Potassium >6.0 meq/L
- EKG may however be normal despite significant Hyperkalemia
- When significant EKG changes are present, pursue aggressive Hyperkalemia Management
- Changes are listed in the classic, textbook description
- However, patient's EKG findings often fail to follow the typical pattern
- EKG changes occur when Serum Potassium >6.0 meq/L
- Initial
- T Waves peaked or Tented (increased amplitude) in V2, V3, II, III
- Next
- ST depression
- First degree AV Block (PR Interval increases)
- QT Interval shortening
- Next (ominous harbinger)
- QRS Duration widening (>110 msec)
- Loss of P Wave (Junctional Rhythm)
- Sine Wave appearance
- New Bundle Branch Block
- Final
- Biphasic wave (sine wave) QRS and T fusion
- Severe Bradycardia
- Imminent Asystole, Ventricular Tachycardia or Ventricular Fibrillation
- Changes exacerbated by
- Hyponatremia
- Hypocalcemia
- Metabolic Acidosis
- Hypermagnesemia
- Chronic Renal Failure with frequent, recurrent Hyperkalemia
- Change from normal EKG to Cardiac Arrest may be rapid in these patients
VIII. Evaluation: Non-Renal Causes (transcellular shift, Potassium load, Pseudohyperkalemia)
- Serious signs of Hyperkalemia present (EKG, symptoms)
- Urgent Hyperkalemia Management
- Consider Pseudohyperkalemia
- Consider confirmatory testing (re-draw sample)
- Consider exogenous source or transcellular shift
- See Hyperkalemia Causes
- Eliminate causative factors
IX. Evaluation: Decreased renal excetion
- Urine Sodium <25 mEq/L suggests decreased distal renal flow
-
Urine Sodium >25 mEq/L with normal serum Aldosterone
- Primary tubular defects (e.g. RTA-4)
- Obstructive uropathy
- Tubular unresponsiveness to Aldosterone (e.g. SLE, Multiple Myeloma, Sickle Cell Anemia)
- Medications (e.g. Potassium sparing Diuretics, Lithium, Trimethoprim)
-
Urine Sodium >25 mEq/L with low serum Aldosterone and normal serum renin
- Primary Adrenal Insufficiency
- Medications (Heparin, Cyclosporine, ACE Inhibitor, ARB)
-
Urine Sodium >25 mEq/L with low serum Aldosterone and low serum renin
- Hyperglycemia
- Primary renal tubular defects
- Medications (e.g. NSAIDs, Beta Blockers)
X. Management
XI. References
- Gibbs in Marx (2002) Rosen's Emerg Med, p. 1730-1
- Klahr (2001) in Noble (2001) Primary Care p. 1359-62
- Kim (2023) Am Fam Physician 107(1): 59-70 [PubMed]
- Viera (2015) Am Fam Physician 92(6): 487-95 [PubMed]