
II. Definitions
- Vertigo
- Sensation of motion (e.g. room spinning) with Disorientation in space
- Results from stimuli mismatch of three systems: vestibular, visual, somatosensory
III. Epidemiology
- Vertigo is the most common cause of Dizziness (54% of cases)
IV. Pathophysiology
- See Vertigo Causes
-
Peripheral Causes of Vertigo
- Inner ear receptor conditions (e.g. Benign Paroxysmal Positional Vertigo, Meniere's Disease)
- Vestibulocochlear Nerve conditions ( Vestibular Neuronitis)
-
Central Causes of Vertigo (affecting the Brainstem, including the vestibular nuclei and Cerebellum)
- Posterior circulation Cerebrovascular Accident (vertebrobasilar CVA)
- Non-Vascular Central Causes of Vertigo (e.g. Acoustic Neuroma, Brainstem lesions, MS)
V. History: Types by Precipitating or Provocative Event
- Triggered Vestibular Syndrome (TVS)
- Trigger examples: Head movement (e.g. peripheral Vertigo such as BPPV), body position (e.g. Orthostasis)
- Contrast with AVS (see below) which is not triggered (but is worse with certain maneuvers such as head turning)
- Perform Dix-Hallpike Maneuver and Orthostatic Blood Pressure and pulse
- Differential Diagnosis
- Spontaneous Episodic Vestibular Syndrome (EVS)
- Distinct episodes without obvious trigger, and asymptomatic between episodes (as well as often on presentation)
- Perform a careful Neurologic Exam and consider TIA Risk Factors
- Differential diagnosis is broad (more likely vestibular if occurs while supine)
- Acute Vestibular Syndrome (AVS)
- Acute, rapid onset (<1 hour) that is persistent, continuous Vertigo or Dizziness (for weeks to months)
- Vertigo is worsened by (but not triggered by) position change
- Associated with Nystagmus, Nausea or Vomiting, head motion intolerance and gait unsteadiness
- Perform HiNTs Exam
- Differential Diagnosis (unlike TVS, which is triggered by position change, AVS includes CVA)
- Ischemic Posterior CVA
- Consider head imaging (includes MRI for reliable assessment for Posterior Circulation CVA)
- Consider Vertebral Artery Dissection in young patients or recent Cervical Spine manipulation
- Caused by Posterior Circulation in 25% of cases
- Tarnutzer (2011) CMAJ 183(9): E571-92 [PubMed]
- Posterior fossa Hemorrhage
- Medication Causes of Vertigo (responsible for >20% of Dizziness in older patients)
- Vestibular Neuronitis
- Wernicke Encephalopathy
- Closed Head Injury (e.g. Post-Concussion Syndrome, Skull Fracture, Whiplash, Vertebral Artery Dissection)
- Middle Ear Barotrauma (Barotitis Media) or Inner Ear Barotrauma (round or oval window rupture)
- See Scuba Diving
- Ischemic Posterior CVA
- References
- Marcolini (2016) Emerg Med News, 38(12): 1
VI. History: Associated Conditions and Exposures
- Preceding Head Trauma
- Preceding viral illness
-
Hearing Loss or ear fullness (muffled)
- Viral Labyrinthitis (distinguishes from Vestibular Neuronitis)
- Meniere Disease (also with Tinnitus)
- Ototoxic Drug exposure (e.g. Aspirin, Aminoglycosides) or medication exposure
-
Cerebrovascular Accident Risk Factors or symptoms (e.g. Atrial Fibrillation, Diabetes Mellitus, Cardiac Risk Factors)
- Acute Cerebellar Stroke
- Vertebrobasilar Insufficiency
- Acute lateral Medullary stroke (Wallenberg Syndrome)
- Recent neck Trauma or neck manipulation (e.g. chiropractor)
-
Cranial Nerve deficits or facial numbness or weakness
- Acute Cerebellar Stroke
- Vertebrobasilar Insufficiency
- Acute lateral Medullary stroke (Wallenberg Syndrome)
- Vertebral Artery Dissection
- Cranial Nerve VIII tumor (e.g. Acoustic Neuroma) or Cerebellopontine angle tumor
- Encephalitis (e.g. Listeria Encephalitis)
- Ataxia
- Optic Neuritis
-
Horner Syndrome
- Acute lateral Medullary stroke (Wallenberg Syndrome)
- Malnutrition (e.g. Alcoholism, Eating Disorder, malabsorption)
VII. Symptoms
- Vertigo characteristics
- Timing
- Timing of Continuous Vertigo (Acute Vestibular Syndrome or AVS)
- Spontanous Onset (e.g. posterior CVA, Vestibular Neuritis)
- Acute onset with possible waxing and waning course
- Trauma or Toxin Related
- Single episode with discrete onset after exposure
- May last days to weeks even after the exposure is removed
- Spontanous Onset (e.g. posterior CVA, Vestibular Neuritis)
- Timing of Episodic Vertigo (Discrete attacks, contrast with the continuous Vertigo of AVS)
- Triggered Vertigo (e.g. BPPV, Orthostasis)
- Sudden onset Vertigo occurs only with specific head rotation
- Vertigo is absent when at rest without head position changes
- Lasts seconds to minutes
- Spontaneous Episodic Vertigo (Spontaneous Episodic Vestibular Syndrome, e.g. TIA, Meniere Disease, Vestibular Migraine)
- Sudden unprovoked onset even at rest (although may be exacerbated by head position changes)
- Lasts minutes to hours
- May experience residual queasy feeling for days
- Triggered Vertigo (e.g. BPPV, Orthostasis)
- Timing of Continuous Vertigo (Acute Vestibular Syndrome or AVS)
- Modifying Factors
- Provocative
- Change in head position
- Differentiate triggered Vertigo (peripheral Vertigo) from exacerbated continuous Vertigo (possible central Vertigo)
- Change in Posture
- Change in head position
- Palliative
- Rest without head turning
- Supine Position (Orthostasis)
- Provocative
- Associated Symptoms
- Symptoms suggesting other cause of Dizziness (not Vertigo)
VIII. Signs: General
-
Vital Signs
- Orthostatic Blood Pressure and Pulse
- New Hypertension may be a sign of autoregulation in acute CVA
- Cardiovascular Exam
-
Neurologic Exam
- Cranial Nerves
-
Carotid Bruits
- Do not perform Carotid Sinus Massage
- Cerebellar tests
- Rapid Alternating Movements
- Romberg Test
- Unsteadiness is present in central Vertigo with or without eyes open
- Gait Exam
- Walk every patient with Vertigo (impaired gait is predictive of central cause)
- Profoundly abnormal in many central Vertigo cases
- Evaluate prior to discharge to assess Fall Risk
- Complete Head and Neck Exam
- See Nystagmus testing below
- Trauma Exam
- Ear Exam
- Middle Ear Anatomy
- Tympanic Membrane Perforation or erythema
- Tympanic MembraneVesicles: Herpes Zoster Oticus
- Cholesteatoma (Posterior superior aspect of TM)
- Tuning Fork Tests
- Weber Test and Rinne Test
- See Hearing Loss
- Middle Ear Anatomy
- Specific vestibular tests (see below)
- STANDING Algorithm for Acute Vertigo
- Triage tool in the Emergency Department to identify cases of possible central Vertigo
- HiNTs Exam (see below)
- Differentiates peripheral Vertigo from central Vertigo in patients with continuous Vertigo (AVS) and Nystagmus
- Dix-Hallpike Maneuver
- Indicated in episodic, triggered Vertigo
- Positive in Benign Paroxysmal Positional Vertigo
- Transient upbeat or torsional Nystagmus on Dix-Hallpike Maneuver suggests BPPV (posterior canal)
- Transient downbeat Nystagmus on Dix-Hallpike Maneuver suggests BPPV (anterior canal)
- McClure-Pagnini Test (Supine roll test)
- Vestibular Testing for BPPV affecting the lateral canal (horizontal canal)
- Patient lies supine on exam table with clinician stands at patient's head
- Patient's head is turned 90 degrees first to one side and then to the other
- Observe for Nystagmus AND its direction for one minute after each head turn
- Positive Test for Horizontal Canal (Lateral Canal) BPPV
- Canalith Repositioning Procedure (Epley Maneuver)
- First-line management and curative in Benign Paroxysmal Positional Vertigo (BPPV)
- Consider performing instead of Dix-Hallpike Maneuver, as it is also diagnostic, with predictable BPPV provocation
- Orthostatic Blood Pressure (and Heart Rate)
- Consider in episodic triggered Vertigo, when Dix-Hallpike Maneuver is negative
- STANDING Algorithm for Acute Vertigo
IX. Signs: HiNTs Exam
- See HiNTs Exam
- See STANDING Algorithm for Acute Vertigo
- Indications
- Acute Vestibular Syndrome with ongoing Vertigo and Nystagmus at time of exam
- Do NOT use the HiNTs Exam when Nystagmus is absent (no benefit)
- Positive HiNTs Exam Criteria (at least 1 of 3 positive) suggests Cerebellar CVA or Brainstem CVA (100% sensitive, 96% specific)
- See HiNTs Exam (Three-Step Bedside Oculomotor Examination)
- Normal Horizontal Head Impulse Test (no saccade/correction on head rotation) OR
- Nystagmus that changes direction (or Vertical Nystagmus or torsional Nystagmus) OR
- Skew Deviation on Alternate Eye Cover Test in which uncovered eye demonstrates quick vertical gaze corrections
- Head impulse test
- See Horizontal Head Impulse Test (Head Thrust Test, h-HIT)
- Grasp head with both hands
- Rapidly rotate head 20 degrees
- Normally one eye lags in response to maintain forward gaze (other eye will lack corrective saccades)
- Eye will normally make quick saccade movement to catch-up or correct (HiNTs-Peripheral)
- An abnormal test (no saccade), or HiNTs-Central
- Suggests a central cause of Acute Vestibular Syndrome (AVS)
- Saccades may also be absent if the Vertigo has resolved
-
Direction Changing Nystagmus (or Nystagmus that is vertical or torsional)
- See Nystagmus
- Patient follows examiner's finger as they move it slowly in all direction
- Examiner moves finger up, down, left or right and to eccentric positions (off-center)
- Nystagmus should be present in all cases of acute vestibular system whether of peripheral or central cause
- Findings suggestive of peripheral Vertigo
- Horizontal Nystagmus (esp. unidirectional) suggests a peripheral cause (although it does not exclude a central cause)
- Findings suggestive of central Vertigo (e.g. posterior CVA)
- Vertical Nystagmus
- Torsional Nystagmus
- Nystagmus that changes direction
-
Alternate Eye Cover Testing (Test of Skew)
- See Skew Deviation
- Cover and uncover each eye and observe for vertical saccade movements in response
- Identifies Skew Deviation where one eye corrects by looking up and the other by looking down
- Associated with a Head Tilt
- May be associated with Horner's Syndrome
X. Signs: Other Nystagmus Testing
-
Dix-Hallpike Maneuver (Provoked Nystagmus)
- Unreliable in identifying central Vertigo (with Acute Vestibular Syndrome)
- However, may be helpful in Triggered Vestibular Syndrome
- Abnormal in Benign Paroxysmal Positional Vertigo (BPPV) affecting posterior canal
-
McClure-Pagnini Test (Supine roll test)
- See above
-
Visual Fixation
- Observe for Nystagmus while patient fixes their gaze on an object in the room
- Suppression of Nystagmus by Visual Fixation on an object suggests peripheral Vertigo
- Next, place a blank sheet of paper in front of the eyes to prevent Visual Fixation
- Nystagmus is expected to return when Visual Fixation is not possible
- Observe for Nystagmus while patient fixes their gaze on an object in the room
-
Spontaneous Nystagmus (Check with non-fixated gaze)
- Formal testing might include Frenzel Lenses to measure the degree of Nystagmus
- Occlusive Ophthalmoscopy
- Cover one of patient's eyes
- Use ophthalmoscope to focus on the Optic Disk
- Note Nystagmus movements
XI. Precautions: Red Flags (Brainstem or cerebellar cause)
- Brief duration does not exclude Posterior Circulation event (e.g. TIA)
- Vertical Nystagmus or Direction Changing Nystagmus (aside from transient with the Dix-Hallpike Maneuver)
- Skew Deviation
- Normal Horizontal Head Impulse Test
- Severe imbalance with gait Ataxia
- Truncal Ataxia while sitting upright
- Associated neurologic findings
- Hand Incoordination or dysmetria
- Unilateral limb weakness
- Loss of Sensation
- Diplopia
- Dysarthria
- Concurrent changes in taste, Swallowing or speech
- Suggests a Brainstem lesion
- Brainstem lesion (e.g. CVA) that affects Vestibular Function is likely to affect taste, Swallowing and speech
- Vestibular nucleus in close proximity to other CN nucleii in the Brainstem
XII. Labs
- Labs are indicated when central Vertigo is suspected (e.g. Cerebrovascular Accident)
- Labs are rarely useful in the peripheral Vertigo evaluation (<1% of cases)
- Labs are indicated for other causes of Dizziness (e.g. Syncope or Presyncope, chronic comorbidity)
- Complete Blood Count (CBC)
- Chemistry panel (Electrolytes including Potassium and Glucose)
- Thyroid Stimulating Hormone
- Continuous ECG Monitor (14 to 28 days)
XIII. Diagnostics
- Acute Vertigo
- Electrocardiogram indications
- Central Vertigo
- Evaluate for Atrial Fibrillation for thrombosis source
- Other Dizziness evaluation
- Evaluate for Syncope or Presyncope
- Central Vertigo
- Electrocardiogram indications
- Chronic or persistent Vertigo
- Audiogram
- Vertigo with Hearing Loss
- Meniere's Disease suspected
- Electronystagmography (ENG)
- Quantifies and records Nystagmus
- Audiogram
XIV. Imaging: Indications
- Acute Vertigo with suspected central Vertigo
- Emergency department yield on CT Head imaging in undifferentiated acute Vertigo is <2.2%
- In contrast, follow-up MRI demonstrates CVA in 16%
- Reserve imaging for those at risk for CVA and presentations suggestive of central CVA (see red flags above)
- Lawhn-Heath (2012) Emerg Radiol 20(1):45-9 [PubMed]
- Obtain CT/CTA Head and Neck (or MRI/MRA if outside CVA Intervention window)
- Assess for cerebrovascular cause
- Vertebrobasilar infarction or insufficiency
- Labyrinthine artery thrombosis
- Anterior Inferior Cerebellar Artery insufficiency or infarction
- Posterior Inferior Cerebellar Artery insufficiency or infarction
- Subclavian Steal Syndrome
- Emergency department yield on CT Head imaging in undifferentiated acute Vertigo is <2.2%
- Chronic Vertigo with Sensorineural Hearing Loss (or other neurologic deficits)
- Obtain MRI Brain
- Assess for structural abnormality
- Acoustic Neuroma
- Other mass lesion
- Demyelinating disease (e.g. Multiple Sclerosis)
- Chiari Malformation
- Inner ear disruptions (e.g. Fractures, semicicular canal dehiscence)
- May also be seen on CT Head
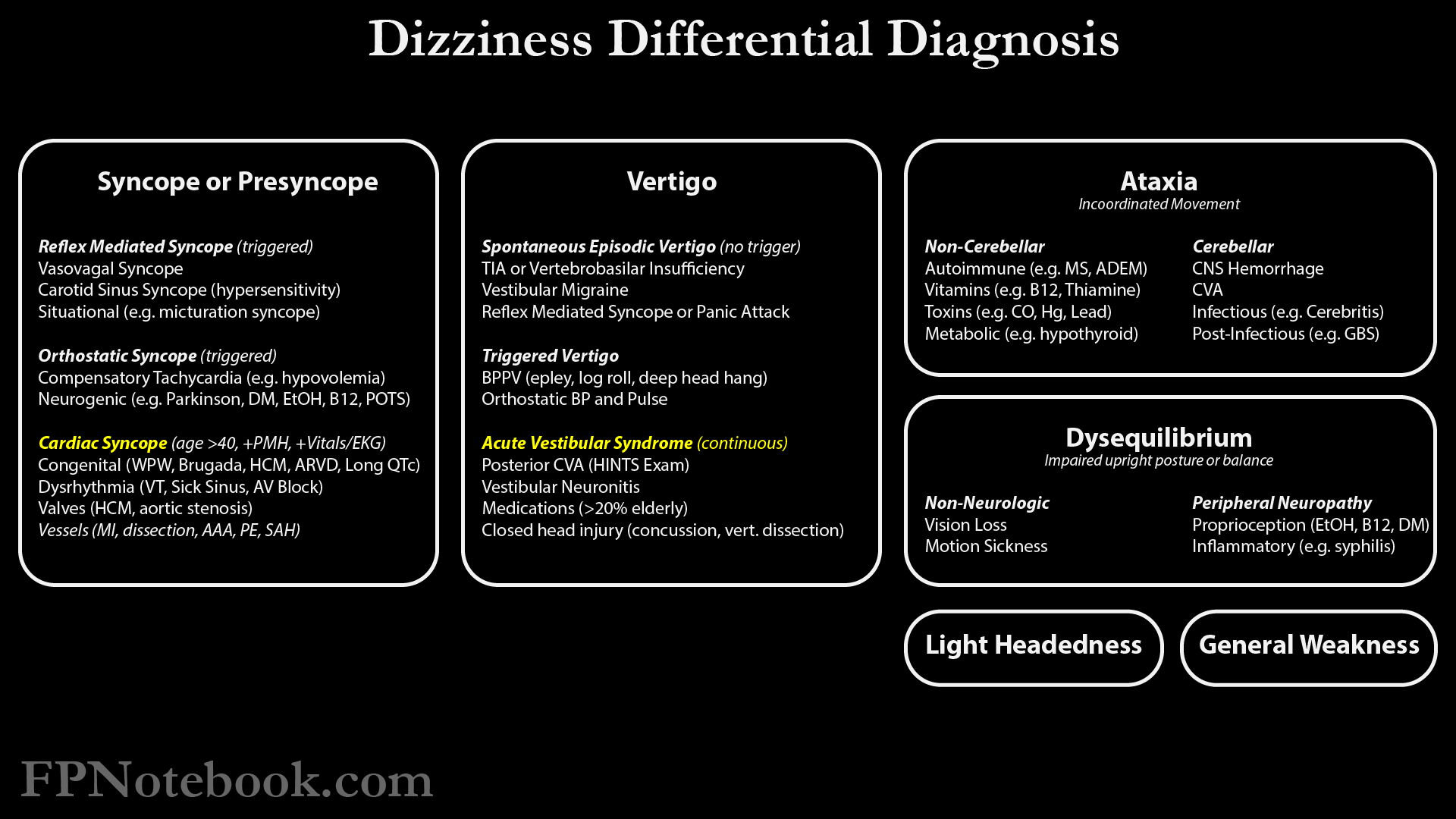
XV. Differential Diagnosis: Dizziness
- See Dizziness Causes
-
Vertigo Causes
- Peripheral Causes of Vertigo
- Central Causes of Vertigo
- Miscellaneous Causes
- Motion Sickness
- Vertigo Caused by Medication
- Psychological cause
- Non-Vertigo cause
- Images
XVI. Evaluation
- Distinguish from non-Vertigo Causes with distinct diagnostic pathways
- Precaution
- Dizziness in older patients may be difficult to categorize (e.g. Presyncope versus Vertigo)
- Syncope or Presyncope
- Dysequilibrium or Ataxia
- Muscle Weakness
- Precaution
- Episodic Vertigo
- Precaution
- Follow continuous algorithm (see below) if symptoms are constant, even if worsened with maneuvers
- Acute Vestibular Syndrome (AVS) symptoms are often made worse with provocative maneuvers
- However, unlike episodic Vertigo, AVS symptoms are still present between episodes
- Triggered Episodic Vertigo
- Perform Dix-Hallpike Maneuver (positive if provokes Vertigo, even if no Nystagmus seen)
- Positive Test: Benign Paroxysmal Positional Vertigo
- Negative Test: Consider Orthostatic Hypotension
- Spontaneous Episodic Vertigo
- Meniere Disease (Hearing Loss, Tinnitus)
- Vestibular Migraine (Migraine Headache, light sensitivity)
- Anxiety Disorder
- Precaution
- Continuous Vertigo
- Consider known exposures
- Medication Causes of Vertigo (causes >20% of Vertigo cases in older patients, esp. if on >5 medications)
- Ear Barotrauma (see Scuba Diving)
- Perform HiNTs Exam
- Positive HiNTs Exam
- Negative HiNTs Exam
- Peripheral Vertigo (e.g. Vestibular Neuronitis)
- Consider exposures listed above (e.g. medications, ear Barotrauma)
- Consider known exposures
XVII. Management
XVIII. References
- Ondrejka (2014) Crit Dec Emerg Med 28(10): 11-7
- Baloh (1999) Postgrad Med 105(2):161-72 [PubMed]
- Knox (1997) Am Fam Physician 55(4):1185-90 [PubMed]
- Labuguen (2006) Am Fam Physician 73:244-51 [PubMed]
- Muncie (2017) Am Fam Physician 95(3): 154-62 [PubMed]
- Rogers (2023) Am Fam Physician 107(5): 514-23 [PubMed]
- Tusa (2005) Neurol Clin 23:655-673 [PubMed]
- Tusa (2003) Med Clin N Am 87:609-41 [PubMed]