
II. Epidemiology
- Accounts for 0.5 to 1% of all Cerebrovascular Accidents
- Female gender in two thirds of cases
- Younger patients (mean age 33 years old)
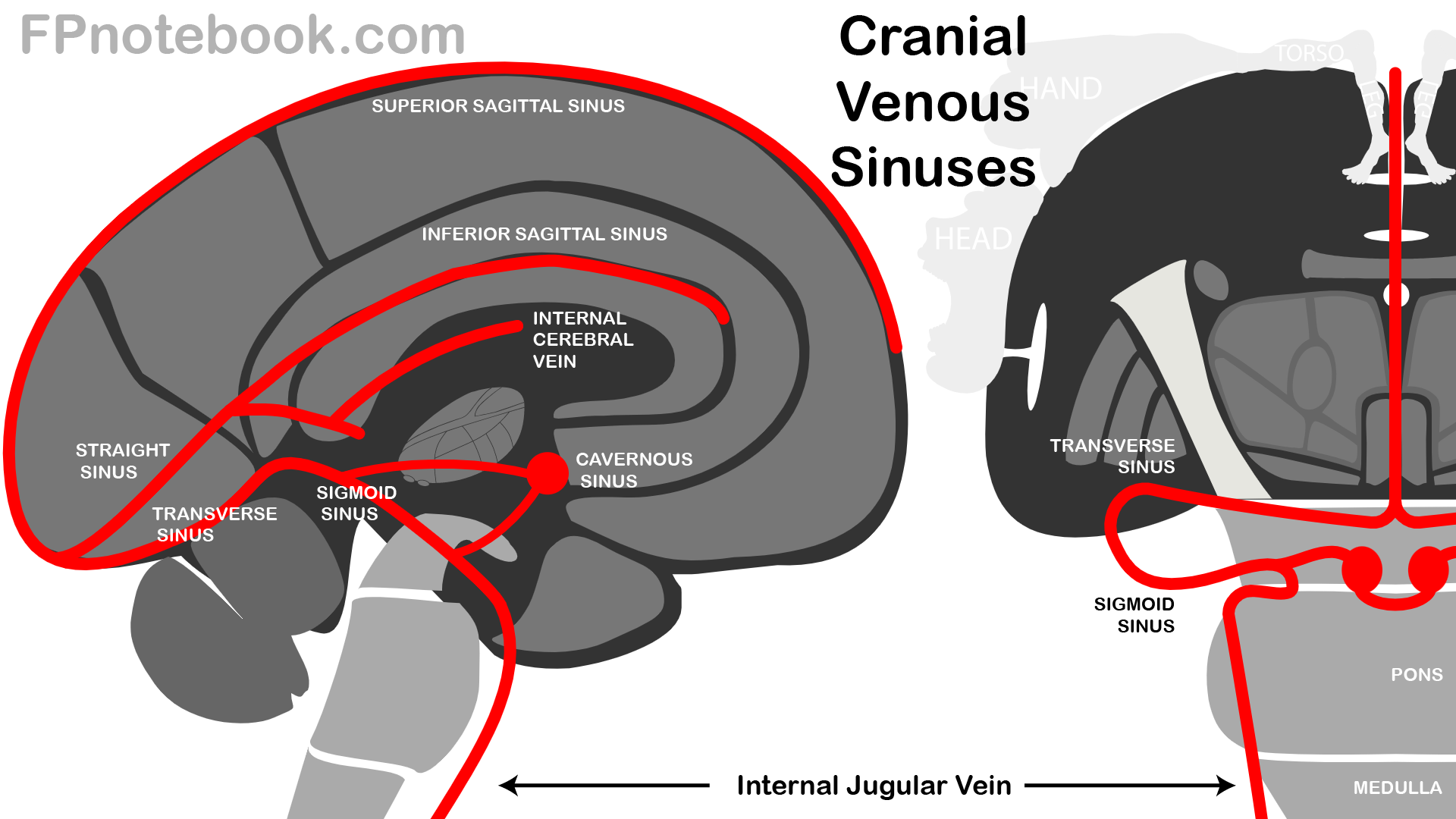
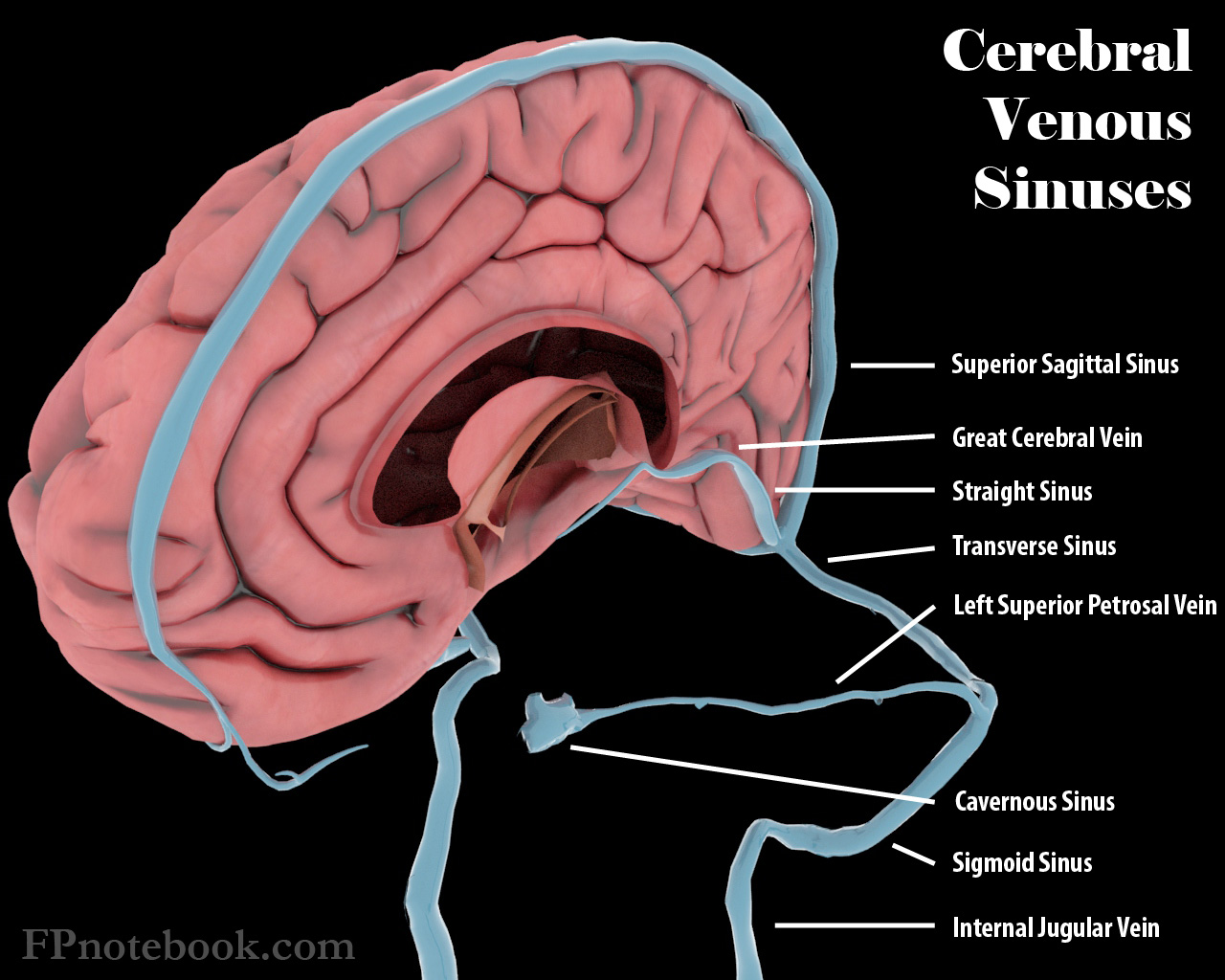
III. Pathophysiology
- See Cerebral Sinus
- Images
- As with other Venous Thromboembolism, virchow's triad applies to pathogenesis (stasis, vessel wall, Coagulopathy)
- Venous obstruction causes increased venous pressure and decreased capillary perfusion
- Initial compensation with venous dilation including collateral veins
- Blood brain barrier is disrupted
- Results in vasogenic edema and possible cerebral Hemorrhage
- Cerebrospinal fluid absorption may also be blocked, increasing Intracranial Pressure
- Results in decreased Cerebral Perfusion Pressure, cerebral ischemia and cytotoxic edema
- Hydrocephalus may develop, with increasing Intracranial Pressure and risk of Cerebral Herniation
IV. Risk Factors
- Precautions
- More than 85% of Cerebral Venous Thrombosis patients have at least one risk factor for thrombosis
- Hormonal
- Oral Contraceptives
- Tamoxifen
- Hormone Replacement Therapy
- Pregnancy or Postpartum State (up to 6 weeks after delivery)
- Most common cause in developed countries
- Accounted for >10% of cases in one study
- Medications
- Asparaginase
- Corticosteroids
- Methotrexate
- Cytotoxic drugs
-
Hypercoagulable Conditions (Thrombophilia, present in 30% of CVT patients)
- See Thrombophilia
- Malignancy (esp. Hematologic Malignancy, myeloproliferative disorder)
- Vasculitis or Inflammation (e.g. Systemic Lupus Erythematosus, Inflammatory Bowel Disease, Behcet's Disease)
- Antiphospholipid Antibody Syndrome
- Hyperhomocysteinaemia (MTHFR gene mutation)
- Factor V Leiden Mutation
- Antithrombin Deficiency
- Protein C Deficiency
- Protein S Deficiency
- G20210A Mutation
- Hematologic Conditions
- Head and Neck Disorders
- Head and Neck Infections (e.g. paramenigeal infections of the ear, sinus or oropharynx)
- Most common cause in developing countries
- Central Nervous System Infections
- Recent neurosurgery
- Closed Head Injury
- Dural AV Fistula or Arteriovenous Malformation
- Head and Neck Infections (e.g. paramenigeal infections of the ear, sinus or oropharynx)
- Miscellaneous Conditions
V. Precautions
- Early diagnosis is key to good prognosis
- Frequently missed diagnosis
- Mimics other acute neurologic conditions
- Requires specific testing in most cases (venogram)
- Consider in atypical Cerebrovascular Accident (CVA)
- Young patients
- Pregnancy or recent postpartum
- Infarcts that cross typical arterial distributions
- Multiple infarcts
- Associated atypical features (Altered Mental Status, Seizures, Headache)
VI. Findings: General
- Findings are specific to venous sinus involved
-
Headache (90% of cases, and only symptom in 25% of cases)
- New or different Headache
- Acute to insidious onset progressive over hours to days (contrast with Thunderclap Headache in SAH)
- Provoked when Increased Intracranial Pressure (e.g. valsalva, coughing)
-
Increased Intracranial Pressure
- Papilledema
- Visual changes
- Nausea or Vomiting
- Focal Findings
- Encephalopathy (esp. deep sinus involvement)
- Altered Mental Status (esp. in elderly)
-
Intracranial Hemorrhage
- Present in up to 40% of CVT patients (secondary to Increased Intracranial Pressure)
- Bilateral parenchymal hemorrhagic lesions or Hemorrhages across multiple arterial territories
VII. Findings: Transverse Sinus Thrombosis
- Accounts for 44 to 73% of cases
- Isolated, noninfectious unilateral thrombosis
- Symptoms may be mild (e.g. Headache) if no infarction
- Seizures
- Contralateral Hemiparesis, hyperreflexia, or spasticity (pyramidal symptoms) may be present
- Left Transverse Sinus (with venous infarction, occluded vein of Labbe)
- Contiguous Sinus extension (e.g. Superior Sagittal Sinus)
- Increased Intracranial Pressure (Intracranial Hypertension)
- Altered Level of Consciousness
- Cranial Nerve Palsy (CN 9-12)
- Cerebral Vein Extension
VIII. Findings: Superior Sagittal Sinus Thrombosis
- Accounts for 39-62% of cases
-
Increased Intracranial Pressure (Intracranial Hypertension)
- Isolated in many cases
- Focal venous infarction related symptoms
- Headache
- Blurred Vision, Vision Loss or Hemianopsia (Visual Field Deficit)
- Nausea or Vomiting
- Cranial Nerve Palsy
- Aphasia
- Hemiparesis or hemi-sensory loss
- Seizures
IX. Findings: Sigmoid Sinus Thrombosis
- Accounts for 40-47% of cases
- Mastoid region pain
- Cranial Nerve Deficit (CBN 6-8)
X. Findings: Deep Venous Cerebral Thrombosis (e.g. Great Cerebral Vein of Galen)
- Accounts for 10-11% of cases
- Altered Mental Status (encephalopathy to coma)
- Motor deficits
- Fluctuating or alternating paresis (or bilateral)
XI. Findings: Cortical Vein Thrombosis (Superficial Cerebral Vein Thrombosis)
- Accounts for 3-17% of cases
- Thrombosis involving superficial veins (superficial middle and anastomotic cerebral veins)
- Seizures
- Focal neurologic deficits depending on distribution of thrombosis
XII. Findings: Cavernous Sinus Thrombosis
- See Cavernous Sinus Thrombosis
- Accounts for 1-2% of cases
- Headache
- Eye Pain
- Chemosis
- Proptosis
- Cranial Nerve Palsy (CN 3, 4, and 6, as well as opthalmic branch CN 5)
- Fever (if septic Thrombophlebitis)
XIII. Labs
- See Cerebrovascular Accident
- Bedside Serum Glucose
- Complete Blood Count
- Basic Metabolic Panel
- Coagulation studies (INR, aPTT)
- Erythrocyte Sedimentation Rate or C-Reactive Protein
- Serum Troponin
-
Thrombophilia labs
- Obtain before Anticoagulation initiated (consult neurology, hematology)
- Other testing
- Evaluate for other triggering events (systemic or CNS Infection)
- D-Dimer does not exclude Cerebral Venous Sinus Thrombosis
XIV. Diagnostics
- Electrocardiogram
-
Optic Nerve Sheath Diameter
- Increased diameter is a marker of Increased Intracranial Pressure (Papilledema)
-
Lumbar Puncture
- Consider in suspected Meningitis or Encephalitis
XV. Differential Diagnosis
XVI. Imaging
- Non-Contrast Head CT
- Low Test Sensitivity for Cerebral Venous Thrombosis (~33%)
- Findings consistent with Cerebral Venous Thrombosis
- Delta Sign
- Posterior Superior Sagittal Sinus hyperdensity
- Venous Cerebral Infarction
- Infarct spans more than one arterial perfusion regions
- Diffuse cerebral edema
- Hydrocephalus
- Subarachnoid Hemorrhage (secondary)
- Delta Sign
- CT Venogram (with CT Head)
- Gold standard study for venous cerebral thrombosis
- CTV identifies filling defects
- Similar efficacy to MRV except in Altered Level of Consciousness or encephalopathy (parenchymal lesions)
- Magnetic Resonance Venogram (MRI/MRV)
- As with CT Venogram, gold standard for Cerebral Venous Thrombosis diagnosis
- MRV is preferred over CT venogram for patients with Altered Level of Consciousness or encephalopathy
- Suggests possible deep cerebral vein thrombosis (better visualized on MRV)
- General Findings
- DWI hyperintense
- Cerebral venous wall enhancement
- Thrombosed sinuses with decreased or absent flow
- Findings vary by timing from onset
- Week 1: T1W/T2W isointense to hypointense
- Week 2: T1W/T2W hyperintense
XVII. Management
- Consult Neurosurgery and Stroke Neurology
- Consult hematology in suspected Thrombophilia
- Initiate Low Molecular Heparin (e.g. Lovenox) which is preferred over Unfractionated Heparin
- Use Unfractionated Heparin in Unstable Patients who may require invasive procedure
- Initiate Anticoagulation with Warfarin with INR target 2-3 for 3-12 months
- Limited evidence for DOACs in CVT as of 2020, and therefore Warfarin is preferred
- Dabigatran (Pradaxa) also has some evidence for use
- First episode of CVT: 3-6 months (6-12 months if no known risk factor)
- Continue Anticoagulation lifelong for recurrent CVT
- Endovascular intervention considered in decompensating or refractory cases
- Manage Increased Intracranial Pressure
- See Acute Severe Intracranial Pressure Management
- Acute monitoring by neurosurgery if risk of Increased Intracranial Pressure
- Cerebral Herniation is the most common cause of death in acute Cerebral Venous Thrombosis
- Manage Seizures
- Antiepileptic drugs are indicated for clinical evidence of Seizures and are continued for >=1 year
XVIII. Complications
- Persistent Focal Neurologic Deficits
- Hydrocephalus and Increased Intracranial Pressure
- Cerebral Herniation
-
Seizures
- Seen in up to 44% of cases in early Cerebral Venous Thrombosis (up to 30% present with Seizure)
- Seizure does not predict prognosis or mortality
- Kalita (2012) Seizure 21(8): 639-42 +PMID:22840965 [PubMed]
XIX. Prognosis
- Mortality: 4.3% in 2004
- Decreased from 50% in 1967, likely due to early recognition and improved diagnostics
- Recurrent Venous Thrombosis risk off of Anticoagulation
- Recurrent Cerebral Venous Thrombosis (>50% who recurr, do so in first year)
- Within first year: Up to 15% recurrence rate
- After first year: 2-7% recurrence per year
- Recurrent Venous Thromboembolism (e.g. DVT, PE): 4-7% per year
- Recurrent Cerebral Venous Thrombosis (>50% who recurr, do so in first year)
- Poor prognostic factors
- Age >35 years old
- Fever
- Altered Level of Consciousness or Coma
- Increased inracranial pressure or Papilledema
- Focal Neurologic deficits
- Banakar (2017) J Neurosci Rural Pract 8(2):204-8 +PMID:28479793 [PubMed]
XX. References
- Alfalasi (2022) Crit Dec Emerg Med 36(3): 3-6
- Lively and Clare (2022) Crit Dec Emerg Med 36(5): 4-10
- Marcolini and Swaminathan in Herbert (2021) EM:Rap 21(2): 5-7
- Ulivi (2020) Pract Neurol 20:356-67 [PubMed]