
II. Physiology: General
-
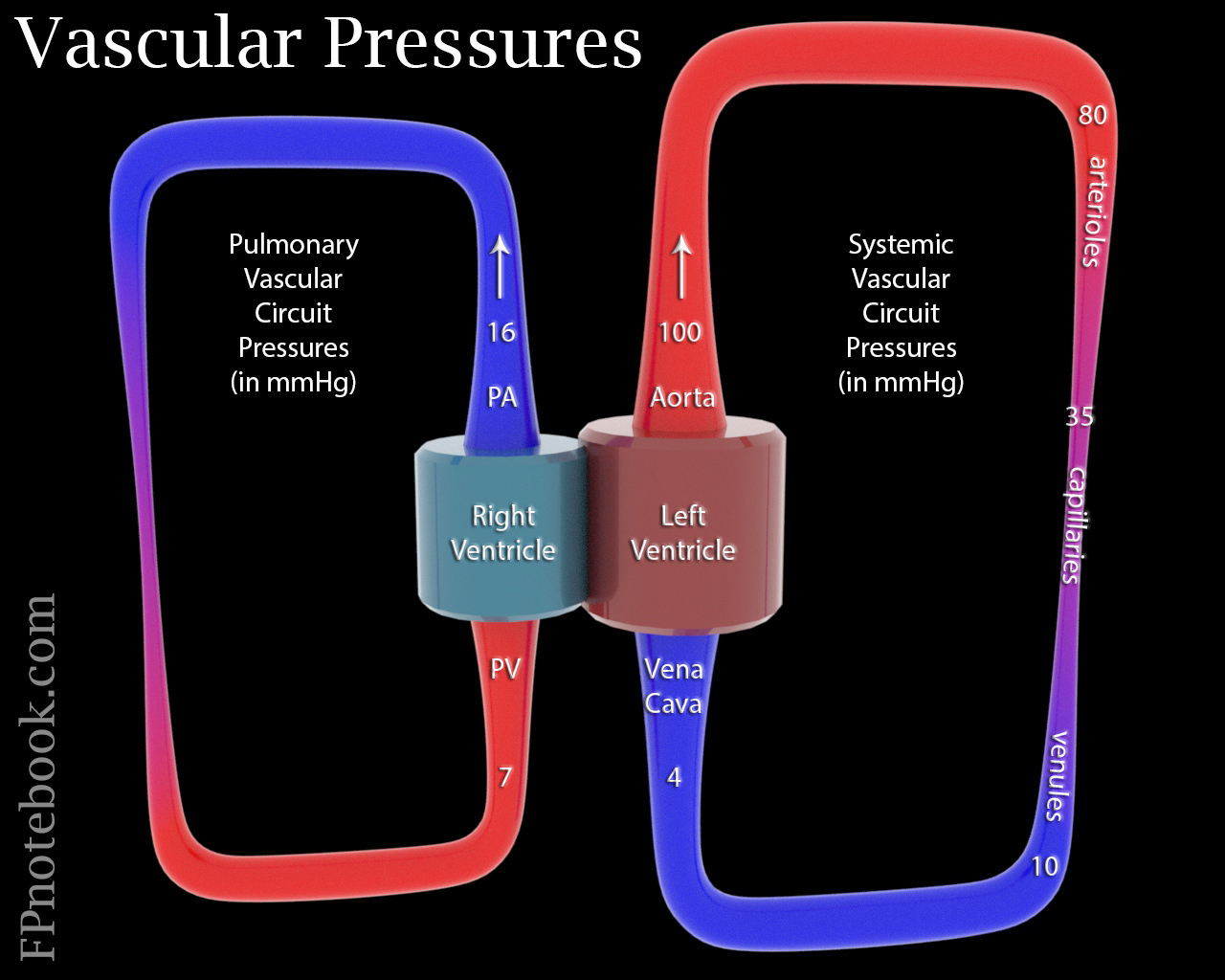
Blood Pressure follows a pressure gradient decreasing as blood enters smaller and smaller vessels (allows for forward flow)
- Mean systolic Blood Pressure drops from 100 mmHg in aorta to <80 in arterioles, <35 in capillaries, <10 in venules
- Forward flow is also maintained by venous valves and Muscle Contractions
- Mean Blood Pressure is lower in the right circulation (16 mmHg pulmonary artery, 7 mmHg right atrium)
- Pulmonary artery pressures are lower in the superior lung fields than inferior lung fields due to gravity
- Overall Blood Flow
- Blood Flow increases with the increasing difference between the pressures at start and ends of vascular circuit
- Blood Flow is impacted primarily by Cardiac Output and Peripheral Vascular Resistance
- Blood Flow is impacted by normal secondary factors
- Lung inspiration (and negative chest pressure) increases venous return
- Skeletal Muscle Contraction
- Isometric Exercise (constant Muscle length) increases Vasoconstriction and Blood Pressure
- Isotonic Exercise (shortening Muscle length) decreases Vasoconstriction and Blood Pressure
- Venous pooling (e.g. prolonged standing)
- Blood Flow is impacted by chronic disease states
- Atherosclerosis with vessel narrowing
- Angiogenesis (prolonged tissue Hypoxia such as vascular disease)
- Blood viscosity (increased in Polycythemia Vera)
- Edematous States (Blood Volume lost to interstitial fluid, e.g Nephrotic Syndrome)
- Images
- Mean systolic Blood Pressure drops from 100 mmHg in aorta to <80 in arterioles, <35 in capillaries, <10 in venules
-
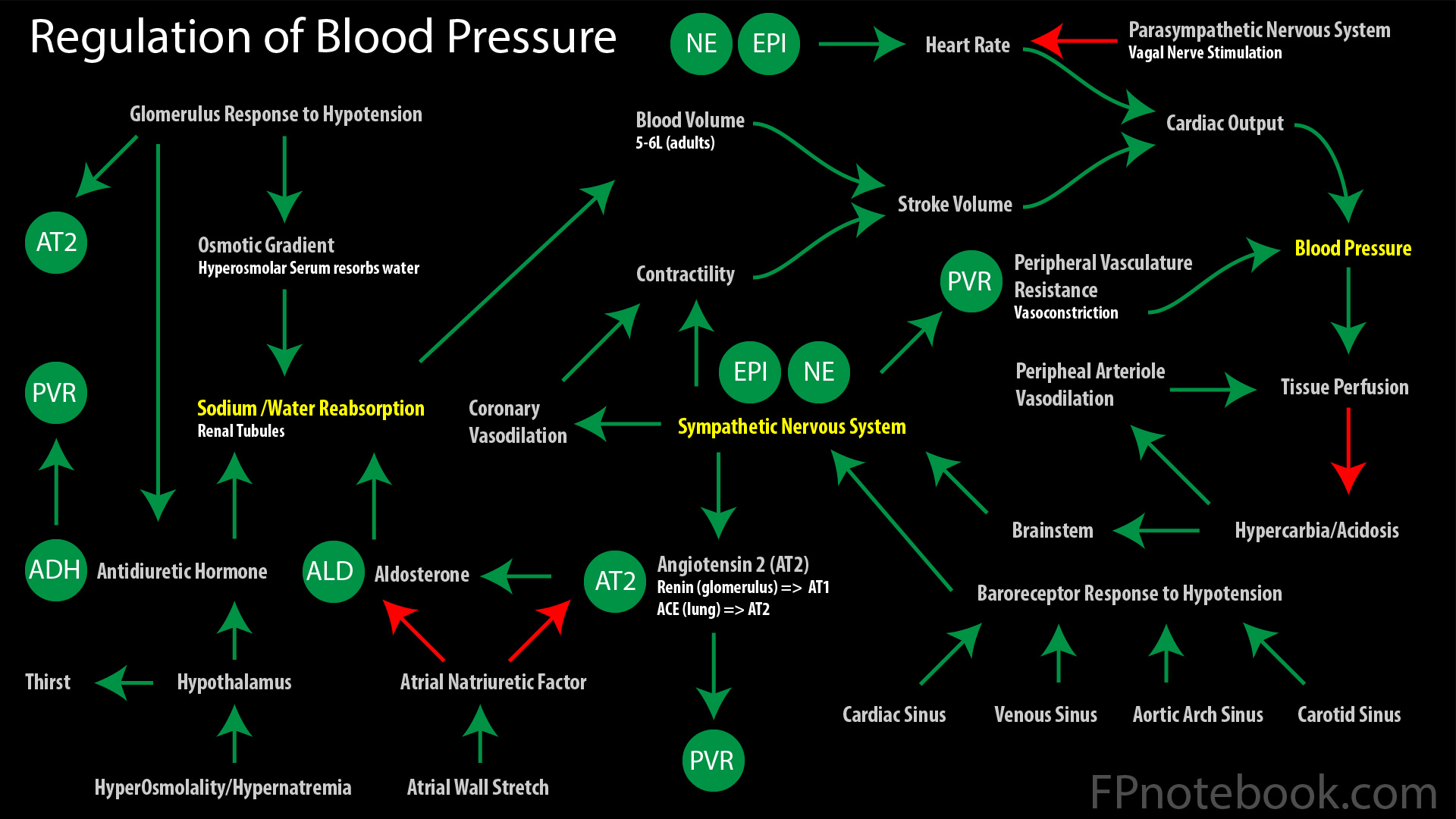
Blood Pressure is maintained by a combination of Peripheral Vascular Resistance and Cardiac Output
- Peripheral Vascular Resistance (vascular tone and Vasoconstriction, Afterload)
- Diastolic Blood Pressure reflects vascular tone
- Vasoconstriction (increased by ADH, Renin/Angiotensin, Aldosterone, Sympathetic Agonists)
- Also increased with stiff, non-compliant vessels (aging) and increased blood viscosity
- Cardiac Output
- Systolic Blood Pressure reflects Cardiac Output
- Cardiac Output = (Heart Rate) x (Stroke Volume)
- Heart Rate is suppressed at baseline by the Parasympathetic System (Vagus Nerve, vagal tone)
- Stroke Volume is dependent on cardiac contractility
- Blood Volume (5-6 L in adults, increased by ADH, Aldosterone)
- See Sodium and Water Homeostasis
- Venous return (Preload) is directly correlated with Stroke Volume (to a maximum)
- Sympathetic Nervous System stimulation
- Increases Heart Rate, contractility, Vasoconstriction via Epinephrine, Norepinephrine
- Stimulates the Renin-Angiotensin System and Aldosterone release
- Images
- Peripheral Vascular Resistance (vascular tone and Vasoconstriction, Afterload)
III. Physiology: Mediators of Blood Pressure Control
- Blood Carbon Dioxide and pH
- Hypercarbia and acidosis stimulate Brainstem with resulting increased sympathetic activity
-
Serum Osmolality
- Increased osmolality and Hypernatremia act at Hypothalamus to increase ADH release
- Increases Sensation of thirst (Hypothalamus mediated)
- Increased Serum Osmolality also acts at renal tubules to reabsorb water
- Heart detection of Blood Volume
- Stroke Volume
- Cardiac contractility increases with Stroke Volume until a maximum (Starling's Law)
- Atrial Natriuretic Factor (ANF)
- Atrial wall stretches with increased Blood Volumes and releases ANF
- ANF acts to decrease fluid volume
- Increases renal tubular Sodium (and water) excretion
- Increases GFR (afferent arteriole vasodilation via relaxed Mesangial Cells)
- Suppresses plasma renin and Aldosterone release
- Stroke Volume
-
Peripheral Vascular Resistance
- Vasoconstriction increases with ADH, Renin/Angiotensin, Aldosterone, Sympathetic Agonists)
- Blood Flow decreases with Vasoconstriction
- Decreases in vessel radius result in exponentially reduced flow (Poiseuille Equation)
- Arteriosclerosis with vessel narrowing also decreases flow
- Sympathetic-mediated Vasoconstriction selectively affects tissue perfusion
- Peripheral vascular response to local mediators
- Mediators of Arteriolar Dilation (and other vasodilation)
- Increased peripheral acid (Hydrogen Ion, carbon dioxide, Lactic Acid)
- Increased Electrolytes (magnesum, Potassium)
- Decreased Calcium
- Vasoactive agents (Adenosine, bradykinin, Histamine, nitric oxide)
- Increased Serum Osmolality
- Tissue Hypoxia
- Other mediators with mixed effects
- Mediators of Arteriolar Dilation (and other vasodilation)
- Baroreceptors
- Baroreceptor distribution
- Venous baroreceptors
- Cardiac baroreceptors
- Carotid Sinus Baroreceptor (via CN 9, Glossopharyngeal Nerve)
- Aortic Arch Sinus Baroreceptor (via CN 10, Vagus Nerve)
- Baroreceptors fire Nerve Impulses at baseline to suppress Blood Pressure
- Baroreceptors detect vascular pressure changes (Hypertension, Hypotension)
- Normal or high Blood Pressure (baroreceptors fire)
- Parasympathetic System is stimulated (e.g. Vagus Nerve stimulation)
- Sympathetic System inhibited (e.g. decreased Catecholamines, ADH)
- Hypotension (decreased baroreceptor firing)
- Parasympathetic System is suppressed (e.g. decreased Vagus Nerve activity)
- Sympathetic System is stimulated (e.g. increased Catecholamines, ADH)
- Baroreceptors (esp. carotid sinus) are sensitive to external pressure
- Carotid Sinus Massage is used as a Vagal Maneuver (e.g. PSVT) to slow Heart Rate
- Carotid Sinus Hypersensitivity may result in Cardioinhibitory Syncope
- Baroreceptor distribution
IV. Physiology: Autonomic System
-
Parasympathetic System
-
Vagus Nerve
- Depresses Heart Rate (and to a lesser extent contractility) and Blood Pressure
-
Vagus Nerve
-
Sympathetic System
-
Brain Stem and Hypothalamus stimulates Sympathetic Nerves to release Norepinephrine
- Vasoconstriction, esp. venous Vasoconstriction (Alpha 1 Adrenergic Receptor)
- Increased Heart Rate and contractility (Beta 1 Adrenergic Receptor)
- Unlike Epinephrine, Norepinephrine has no significant Beta 2 Adrenergic Receptors
-
Adrenal Medulla is stimulated by Sympathetic Nerves to release norepinephine and Epinephrine
- EpinephrineVasoconstricts via Alpha 1 Adrenergic Receptors as does Norepinephrine
- Epinephrine (via Beta 2 Adrenergic Receptors) vasodilates vessels in heart and skeletal Muscle
-
Kidney-based granular cells with Beta 1 Adrenergic Receptors are stimulated by Sympathetic System
- Factors stimulating Granular cell Renin release
- Sympathetic System stimulation (Beta 1 Adrenergic Receptors)
- Low Blood Pressure (direct effects)
- Macula Densa detects low Sodium concentration in the renal tubule
- Low Sodium in the renal tubule occurs in hypovolemic states with decreased GFR
- Renal tubule stasis allows for greater Sodium without water absorption
- Macula densa releases Prostaglandins in response
- Prostaglandins dilate renal afferent arteriole and increase GFR
- Prostaglandins stimulate renin release (increases Sodium AND water reabsorption)
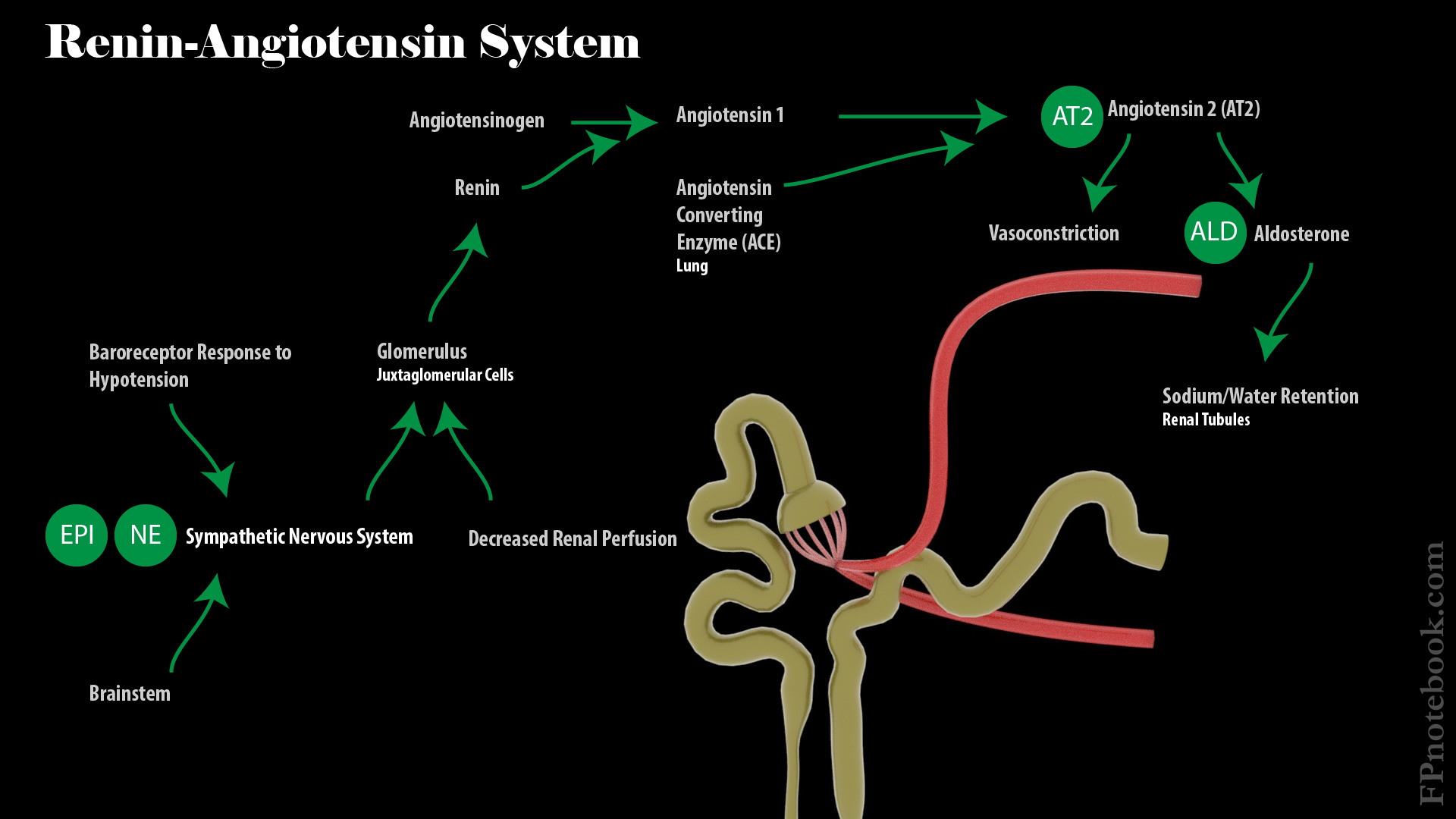
- Renin secreted from renal granular cells and results in Angiotensin 2
- Renin converts Angiotensinogen to Angiotensin 1
- Angiotensin Converting Enzyme (ACE) in pulmonary capillaries converts Angiotensin 1 to 2
- Angiotensin 2 stimulates Vasoconstriction and Adrenal CortexAldosterone release
- Aldosterone stimulates Sodium (and water) reabsorption from renal tubules
- Factors stimulating Granular cell Renin release
-
Brain Stem and Hypothalamus stimulates Sympathetic Nerves to release Norepinephrine
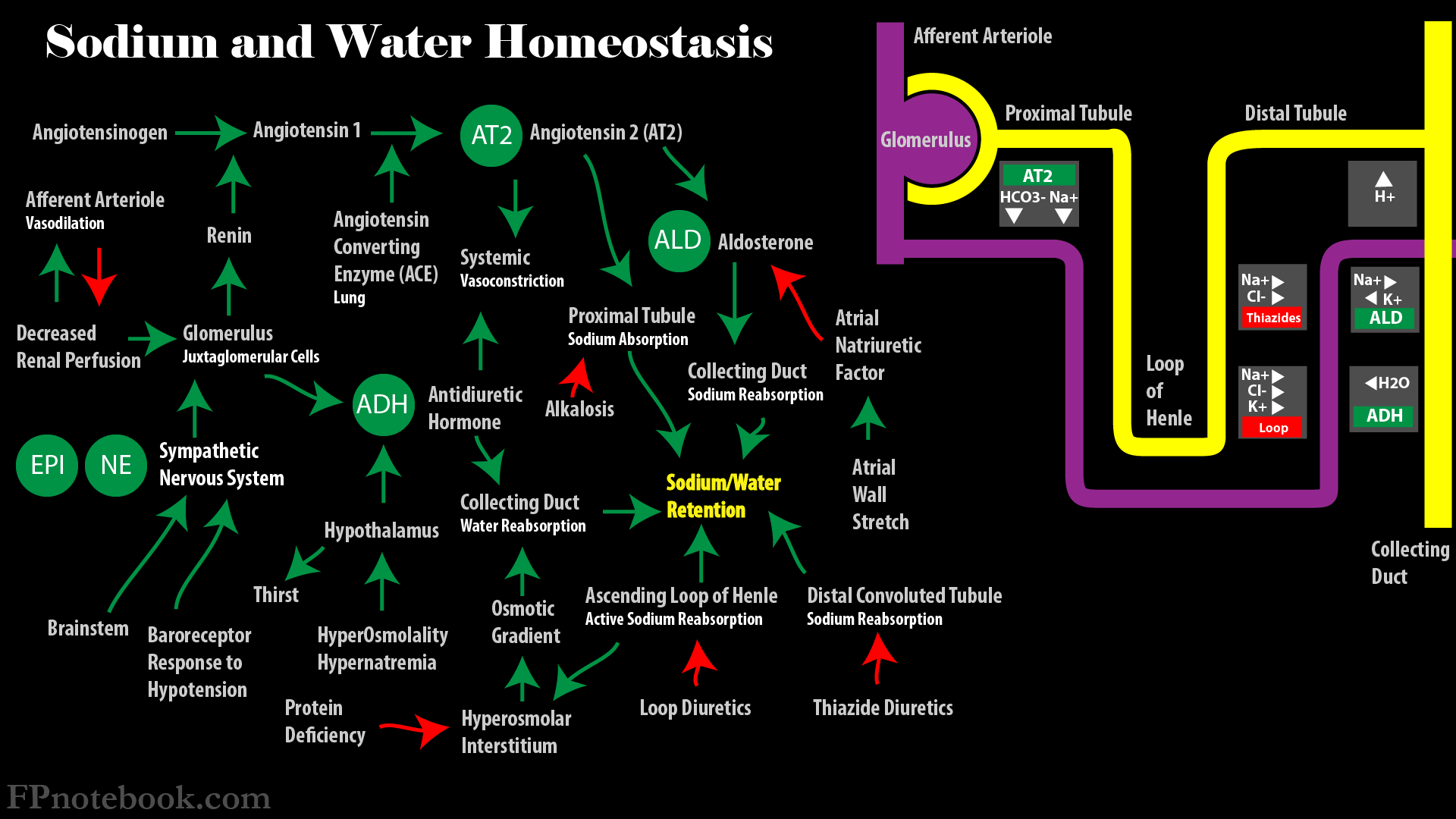
V. Physiology: Sodium and Water Homeostasis
- See Sodium and Water Homeostasis
- Images
-
Antidiuretic Hormone (ADH, Vasopressin)
- Mediators
- Released from Hypothalamus in response to increased Serum Osmolality
- ADH release is inhibited by Alcohol
- Effects
- Increases water reabsorption from renal tubules
- Increases Vasoconstriction and Peripheral Vascular Resistance
- Mediators
- Glomerulus
- Blood Pressure
- High pressures entering glomerulus (afferent arteriole) drive more fluid into urine
- Low Blood Pressures entering glomerulus result in retention of water
- Osmotic pressure
- Serum hypoosomolality (Fluid Overload) results in greater fluid gradient into urine
- Serum Hyperosmolality (Dehydration) attracts fluid back into circulation
- Serum contains large Proteins (esp. albumin) that do not normally cross the glomerulus
- Large Proteins maintain an osmotic pressure gradient into the serum
- In nephropathy (e.g. Nephrotic Syndrome), large Proteins do cross the glomerulus
- Resulting hypoproteinemia results in Interstitial Edema (following osmotic gradient)
- Glomerulus permeability
- Glomerular permeability decreases with decreased glomerular surface area
- Glomerular capillary Mesangial Cells contract in response to ADH and Angiotensin II
- On Mesangial Cell contraction, glomerular surface area is reduced
- Reduced glomerular surface area results in less fluid filtration across the glomerulus
- Blood Pressure
VI. Pathophysiology
- Disordered mechanisms of Blood Pressure regulation
- Inadequate fluid volume
- Inadequate Renal Function
- See Renal Failure
- Inadequate Cardiac Function
- See Cardiogenic Shock (e.g. Congestive Heart Failure)
- Endocrine Disorders
- Antidiuretic Hormone (ADH)
- Diabetes Insipidus (ADH decreased)
- Syndrome Inappropriate ADH Secretion or SIADH (ADH Increased)
- Hyperaldosteronism
- Pheochromocytoma
- Antidiuretic Hormone (ADH)
-
Hypotension
- See Hypotension
- See Syncope
- See Drug-Induced Hypotension
-
Shock
- Hypovolemic Shock (Hemorrhagic Shock, Dehydration, Diabetic Ketoacidosis, Diabetes Insipidus)
- Distributive Shock (Septic Shock, Neurogenic Shock, Anaphylaxis)
- Cardiogenic Shock (Congestive Heart Failure, Cardiomyopathy, Cardiac Contusion, valvular rupture)
- Obstructive Shock (Tension Pneumothorax, Pericardial Tamponade, massive Pulmonary Embolism)
- Transient Hypotension
-
Hypertension
- See Hypertension
-
Secondary Hypertension
- Vascular (Aortic Coarctation, Renal Artery Stenosis)
- Endocrine (Hyperaldosteronism, Pheochromocytoma, Cushing's Disease, Hyperparathyroidism, Hyperthyroidism)
- Miscellaneous (Medication Causes of Hypertension, Obstructive Sleep Apnea, Preeclampsia)
- Generalized Edema
VII. Management: Hypertension
- See Hypertension Management
- See Hypertensive Emergency
- Agents that modify fluid balance
- Diuretics (e.g. Loop Diuretics, Thiazide Diuretics)
- Aldosterone Antagonist (e.g. Spironolactone, Eplerenone)
- Aldosterone blockade results in Sodium (and water) excretion, and Potassium retention
- Agents that modify vascular tone
- Sympathetic activity
- Alpha Adrenergic Central Agonist (e.g. Clonidine) inhibits sympathetic outflow
- Decreases Peripheral Vascular Resistance (via vasodilation) and decreases Heart Rate
- Alpha Adrenergic Antagonist (e.g. Terazosin, Prazosin)
- Block sympathetic stimulation of vascular Smooth Muscle resulting in vasodilation
- Alpha Adrenergic Central Agonist (e.g. Clonidine) inhibits sympathetic outflow
- Direct Vasodilators
- Calcium Channel Blockers
- Inhibits Calcium influx into Smooth Muscle Cells resulting in vasodilation
- Calcium Channel Blockers
- Renin-Angiotensin System
- Angiotensin Converting Enzyme Inhibitor (ACE Inhibitors)
- Blocking ACE activity (lungs), blocks conversion of Angiotensin 1 to Angiotensin 2
- Decreased Angiotensin 2 results in vasodilation and decreased Aldosterone release
- Angiotensin Receptor Blockers (ARB)
- Blocks Angiotensin 2 receptors with similar result as with ACE Inhibitors
- Angiotensin Converting Enzyme Inhibitor (ACE Inhibitors)
- Sympathetic activity
- Agents that modify cardiac activity (contractility and Heart Rate)
- Beta-1 Adrenergic Antagonist or Beta Blockers (e.g. Metoprolol)
- Decrease cardiac contractility and Heart Rate
- Beta-1 Adrenergic Antagonist or Beta Blockers (e.g. Metoprolol)
VIII. Management: Hypotension
- See Shock
-
Hemorrhagic Shock and Severe Dehydration
- Rapid volume replacement with the lost fluid type
-
Septic Shock
- Fluid Resuscitation with large fluid volume bolus (typically 30 cc/kg)
-
Vasopressors (e.g. Norepinephrine) when fluid Resuscitation fails to raise mean arterial pressure (MAP) > 65 mmHg
- Norepinephrine increases cardiac contractility and Vasoconstriction
- Identification of infection source and early use of Antimicrobial Agents
-
Cardiogenic Shock
- Hypotension in Cardiogenic Shock is among the most difficult acute stabilization tasks
-
Hypotension limits the typical CHF strategy of Preload reduction
- However, noninvasive Positive Pressure Ventilation (e.g. BIPAP) may be tolerated
- BiPAP reduces proload and improves oxygenation without a drop in circulating volume
-
Vasopressors (sympathetic agents) are often required acutely
- Norepinephrine
- Beta 1 Adrenergic ReceptorAgonist (increased contractility)
- Alpha Adrenergic ReceptorAgonist (Vasoconstriction)
- Dobutamine
- Beta 1 Adrenergic Receptor (increased cardiac contractility and Heart Rate)
- Beta 2 Adrenergic Receptor (mild increase in vasodilation)
- Norepinephrine
IX. References
- Goldberg (2014) Clinical Physiology, Medmasters, p. 4-20
- Guyton and Hall (2006) Medical Physiology, p. 195-231