
II. Epidemiology
- Accounts for 10% of Vaginitis
-
Prevalence
- General gynecology clinics: 13-23%
- Prostitutes: 75%
- Increasing Prevalence in asymptomatic women over age 45 years old
- More common in women with HIV Infection
- Screen women with HIV yearly
- Transmission
- Sexually Transmitted Disease
- Trichomonas is the most common non-viral Sexually Transmitted Infection
- Men are asymptomatic in 90% of cases
- Often transmitted with Gonorrhea and Chlamydia
- Rarely transmitted by moist cloths
- Sexually Transmitted Disease
III. Etiology
- Protozoan infection
IV. Risk Factors
- Multiple sexual partners
- Sexually Transmitted Infections
- Unprotected Intercourse
- Illicit Drug use
- Tobacco Abuse
V. Symptoms
- Asymptomatic in 25-44% of women
- Copious, yellow-green or grayish-green Vaginal Discharge (variably present)
- Fishy odor to discharge (variably present)
- Frothy discharge (Carbon dioxide bubbles)
- Sensitivity: 10%
- Specificity: 70%
- Vulvar and vaginal Pruritus with irritation and edema
- Dysuria (20%)
VI. Signs
- Vulvar edema and erythema
- Tender vaginal or vulvar ulcerations
- Strawberry Cervix (2-3% of cases)
- Punctate Hemorrhages or Petechiae
- Telangiectasia
VII. Lab
- Vaginal pH > 5.0
-
KOH Preparation
- Sniff Test positive
- Fishy odor to discharge when KOH added (often negative)
- Sniff Test positive
-
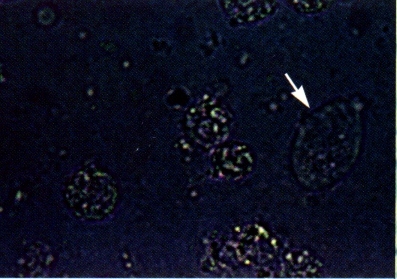
Wet Preparation (from vaginal vault, not endocervix)
- Read slide immediately
- Motility wanes quickly, over minutes
- Trichomonad shape morphs from pear-shaped to round with slide drying
- Motile pear shaped Trichomonads with flagella exiting from tapering end (70%)
- Twice the size of White Blood Cells (WBC)

- Efficacy
- Test Sensitivity: 60-70%
- Read slide immediately
- Specific diagnostic tests
- DNA Testing is preferred for Trichomonas diagnosis, and can be added to DNA probe and liquid pap
- Preferred over microscopy in symptomatic or high risk women
- Nucleic Acid Amplification Test (NAAT) Sensitivity: >95%
- May be added to GC/Ch DNA probe or liquid pap
- Rapid swabs are also available, with Test Sensitivity 80-90%
- Available as point-of-care clinic based tests
- Test Sensitivity: 83%
- Test Specificity: >97% (False Positives are a concern in regions of low Prevalence)
- BD Affirm VPIII Microbial Identification Test (Nucleic Acid probe)
- Osom Trichomonas Rapid Test (immunochromatographic)
- DNA Testing is preferred for Trichomonas diagnosis, and can be added to DNA probe and liquid pap
- Other testing
- Gram Stain
- White Blood Cells over 10 per high powered field
- Culture of Trichomonas vaginalis (replaced with DNA probes)
- Grown on modified Diamond media
- Gram Stain
VIII. Associated Conditions
IX. Management
-
General
- Treat Sexual Partner also
- Metronidazole 500 mg orally twice daily for 7 days is most effective for male partners
- However, Metronidazole 2 g orally for one dose is recommended in guideline for male partners
- Abstain from intercourse until they and their sexual partners are treated
- Avoid treatment in first trimester of pregnancy
- Avoid intravaginal preparations of Metronidazole or Tinidazole due to low cure rates
- Re-test in 3 months (high risk of reinfection)
- Treat Sexual Partner also
- Non-Pregnant, Non-Lactating Patient
- Metronidazole (Flagyl) 500 mg orally twice daily for 7 days (preferred) OR
- Avoid single Metronidazole (Flagyl) 2 g oral dose (less effective)
- Tinidazole (Tindamax) 2 grams orally for 1 dose
- Teratogenic, Category D (do not use if any risk of pregnancy)
- More expensive than Metronidazole options
- Metronidazole (Flagyl) 500 mg orally twice daily for 7 days (preferred) OR
- Pregnant (after first trimester, and preferred after 37 weeks)
- Metronidazole (Flagyl) 2 g orally for 1 dose OR
- Metronidazole (Flagyl) 500 mg orally twice daily for 7 days
-
Lactation
- Metronidazole (Flagyl) 2 grams orally for 1 dose
- Discontinue Lactation for 24 hours after dose
- Persistent or Recurrent Cases
- Retreat both the sexual partner and the patient
- Metronidazole 500 mg orally twice daily for 7-14 days
- Metronidazole 2g orally daily for 3 days (for up to 7 days)
- Metronidazole gel 5g PV bid for 5 days
- Povidone-Iodine Suppository PV bid for 14 days
- Clotrimazole 100 mg vag tab PV qhs for 7 days
- Tinidazole 2 g orally daily for 5 days
- Teratogenic, Category D (do not use if any risk of pregnancy)
- Paromomycin (Humatin) 5g intravaginally qd x14 days
- Higher rate of Vulvitis and local ulceration
- Secnidazole (Solosec) 2 g orally for 1 dose
- Expensive in 2021 ($270 for one dose)
- (2021) Presc Lett 28(9): 49-50
X. Complications
- HIV Infection and transmission risk
- Preterm Labor
- Associated with concurrent other Sexually Transmitted Infections
XI. References
- Mandell (2000) Infectious Disease, Churchill, p. 2894-7
- (1998) MMWR Morb Mortal Wkly Rep 47:1-115 [PubMed]
- Epling (2001) Am Fam Physician 64(7):1241-4 [PubMed]
- Workowski (2006) MMWR Recomm Rep 55:1-94 [PubMed]