
II. Definitions
- T Wave
- EKG electrical signal following the ST Segment
- Represents repolarization of the ventricular Muscles
III. Findings: Normal
- Upright: I, II, V3, V4, V5, V6
- Inverted: aVR
- Variable (upright, inverted or biphasic): all other leads
- Increased Amplitude: aVL and aVF (if QRS over 5 mm)
- Shape: Asymmetrical
- An upright T Wave normally rises gradually, and falls with a steeper slope
IV. Findings: T Wave Shape
- Smooth: Normal
- Notched: Pericarditis
- Pointed: Myocardial Infarction
- T Wave Alternans
- Upright T Wave alternates with inverted T Wave on every other beat
- May be associated with Prolonged QTc (as well as predisposing Hypokalemia or Hypocalcemia)
- Marker of myocardial electrical instability
- Ominous finding that heralds ventricular Dysrhythmia, Torsades de Pointes or Cardiac Arrest
V. Findings: T Wave Height
- See Tall P Waves below
- Normal
- Limb leads: <6 mm
- Precordial leads: < 10 mm
- T-Wave Flattening (T Wave height -1 to 1 mm)
- Post-coronary ischemic event
- Hypokalemia
- Digitalis
VI. Causes: Tall, peaked, prominent or Hyperacute T Wave Causes
-
Hyperkalemia
- See Hyperkalemia Related EKG Changes
- T Waves are narrow, tall and symmetric
- T Waves may be inverted (negatively peaked)
-
Myocardial Infarction or Myocardial Ischemia
- T Waves are less tall and more wide and asymmetric than in Hyperkalemia
- De Winter T Wave is a Hyperacute T Wave with J Point depression and consistent with acute LAD Occlusion
- Prominent T Waves often immediately precede ST Elevation in STEMI
- Obtain Serial EKGs
- AHA/ACC consider Hyperacute T Waves in ACS presentation as a STEMI Equivalent (consult cardiology)
- However, grading T Wave size is subjective, and there is no T height calculation that reliably predicts high risk ACS
- T Waves that are as tall or taller than the QRS Complex are significant
- Observe for associated ST deviation >=1mm or dynamic T Wave changes
- AVL T Wave Inversion precedes inferior Myocardial Infarction
- Other Causes of Tall T Waves
- Cerebrovascular Accident
- Acute Pericarditis
- Left Ventricular Hypertrophy
- Early Repolarization
- High voltage EKG
- Left Bundle Branch Block
- Preexcitation Syndrome
- References
- Mattu (2008) Crit Dec Emerg Med 33(12): 11
- Mattu and Swaminathan (2023) EM:Rap, accessed 10/1/2023
- Koechlin (2023) Ann Emerg Med 82(2):194-202 +PMID: 36774205 [PubMed]
- Smith (2023) Ann Emerg Med 82(2):203-6 +PMID: 36872197 [PubMed]
VII. Causes: T Wave Inversion
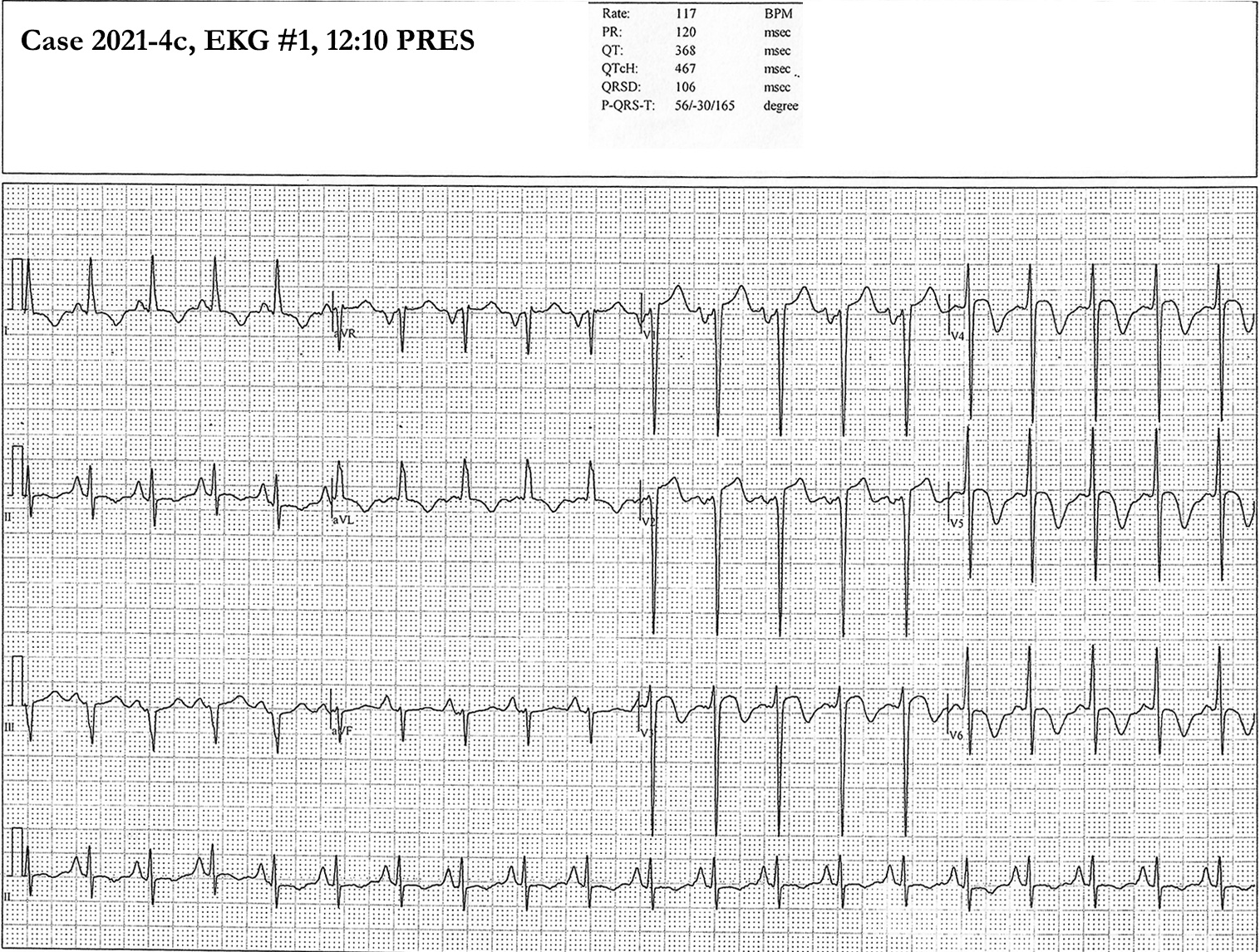
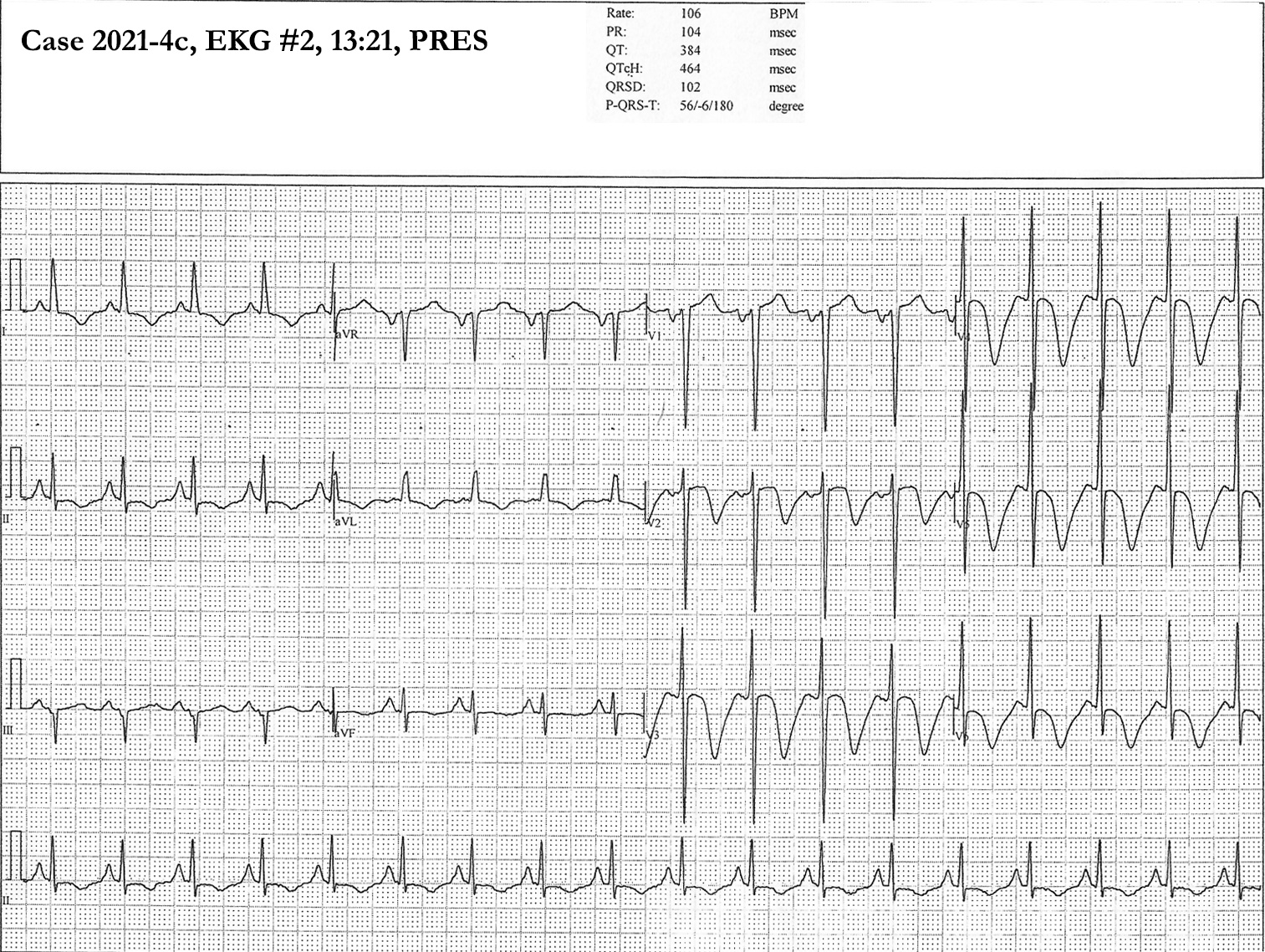
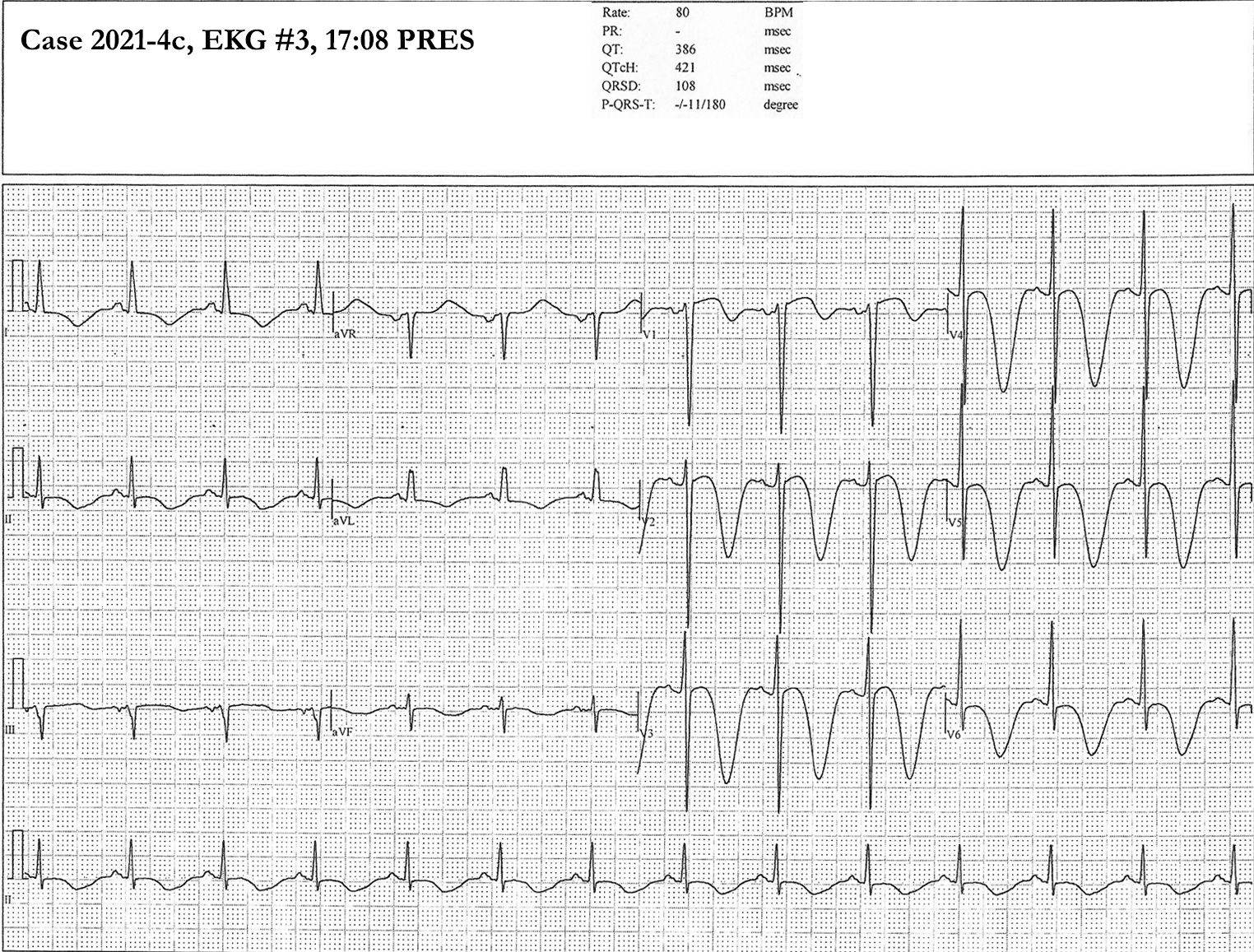
- Very Deep T Wave Inversion (Cerebral T Waves)
- Associated with large Intracranial Hemorrhage (also seen in cerebral edema, Ischemic CVA, PRES)
- Typically in precordial leads, and Inversion may be >20 mm
- May be associated with Prolonged QTc
- Images: Deep Inverted T Waves Precordial in Hypertensive Encephalopathy (PRES)
- References
- Mattu and Brady (2008), EKGs for the Emergency Physician 2, BMJ, London, p. 11, 23
- Mattu (2022) Crit Dec Emerg Med 36(3): 7
- T Wave Inversion (in general)
- Heart Block
- Ischemic Heart Disease with Myocardial Ischemia or infarction
- Bradycardia
- Right Ventricular Hypertrophy
- Right Bundle Branch Block
- Metabolic disturbance
- Takotsubo Cardiomyopathy
- Pulmonary Edema
- Cocaine Use
- Acute CNS events
- References
- T Wave Inversion specific to anterior leads (V1 to V4)
- Juvenile T Wave Pattern
- T Wave Inversion is normal in V1-V3 in age <16 years (athletes and non-athletes)
- Anterior Myocardial Ischemia
- Proximal Left Anterior Descending Occlusion
- See Wellen's Syndrome
- Deeply inverted T Waves or biphasic T Waves in V2-3
- Posterior Myocardial Infarction
- Pulmonary Embolism with right heart strain
- Neurogenic T Waves
- Precedes ischemic cerebrovascular event
- Yamaguchi Syndrome
- Hypertrophic Cardiomyopathy involving the cardiac apex
- Hypokalemia
- Biphasic T Wave in mid-precordial leads
- Mattu (2017) Crit Dec Emerg Med 31(3): 11
- References
- Herbert (2012) EM:RAP 12(1): 12
- Juvenile T Wave Pattern
VIII. References
- Berberian (2023) Crit Dec Emerg Med 37(5): 12-3