
II. Types
- Primary Biceps Tendinitis (5% of cases)
- Inflammation within bicipital groove
- Long head of biceps tendon and sheath
- Secondary Biceps Tendinitis (95% of cases)
III. Risk factors
- Biceps tendon impingement primary causes (impingement under coracoacromial arch)
- Acromion bone spur
- Unfused acromial apophysis
- Coracoacromial ligament thickening
- Biceps tendon impingement secondary causes
- Scapular instability
- Shoulder ligamentous instability
- Lax anterior capsule
- Tight posterior capsule
- Labral tear
- Rotator Cuff Tear
- Osteoarthritic spurs at bicipital groove
- Associated activities at higher risk for acute Tendinitis or chronic overuse Tendinosis
- Repetitive throwing
- Contact Sports
- Swimming
- Gymnastics
- Martial arts
- Secondary inflammation due to Arthritis (tendon originates inside Shoulder joint)
- Rheumatoid Arthritis
- System lupus erythematosus
- Reactive Arthritis
- Septic Arthritis
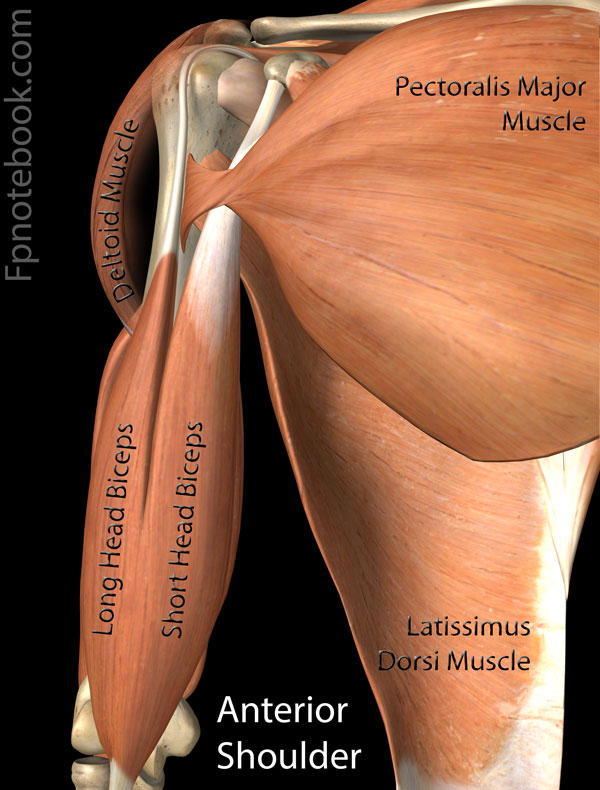
IV. Background: Anatomy
- Images
- Long head of biceps
- Originates at supra-glenoid tubercle (anterior superior aspect adjacent to glenoid fossa)
- Travels laterally through Shoulder joint in front of Humerus
- Descends under the transverse humeral ligament and into the bicipital groove
- Transverse humeral ligament acts as a pulley, reorienting the tendon inferiorly
- Landmarks: Groove lies between greater tuberosity (lateral) and less tuberosity (medial)
V. Symptoms
VI. Signs
- Tenderness over bicipital groove
- Biceps Tendon Instability may cause a palpable or audible snap on range of motion testing
- Pain limits active and passive range of motion
- Maneuvers that stretch biceps elicit pain
- Forceful external rotation with abduction (shifts bicipital groove to a posterolateral position)
- Arm extension with elbow extended
- Yergason Test
- Speed's Test
VII. Differential Diagnosis
- Rotator Cuff Impingement or Rotator Cuff Tear
- Cervical Disc Disease
VIII. Precautions
- Bicipital Tendon Injury is commonly associated with Rotator Cuff Injury or SLAP Lesion
IX. Management
- Acute management (until pain resolves)
- Rest
- Moist heat
- Gentle range of motion
- NSAIDs
- Avoid motion that stretches biceps tendon (especially overhead motion)
- Sling temporarily if needed (but avoid immobility due to risk of Frozen Shoulder)
- Rehabilitation Exercises (start when pain free)
- Step 1: StretchingExercises
- Shoulder specific Stretching: Scapula, Rotator Cuff and Posterior Capsule
- Hamstrings
- Low Back
- Step 2: Strengthening Exercises
- Step 3: Throwing program (athletes)
- Step 1: StretchingExercises
-
Biceps Tendon Injection
- Local Corticosteroid Injection at tendon sheath under Ultrasound guidance (see Shoulder Ultrasound)
- Approached in-plane to linear Ultrasound probe (probe short axis to anterior Shoulder - home position)
- Do not inject within tendon (and avoid circumflex artery within groove)
- May also help differentiate rotator cuff source of pain from primary Bicipital Tendinitis
- Surgery is indicated for failed conservative therapy after 3 months
- Partial Biceps Tendon Rupture (<50%): Debridement
- Debridement of impinging structures
- Ruptured tendon and age <60, athletes or otherwise active: Biceps tenodesis
- Tendon anchored in the bicipital groove
- Ruptured tendon and age over 60 years: Biceps tenotomy
- Biceps tendon removed from glenohumeral joint without loss of function
- Partial Biceps Tendon Rupture (<50%): Debridement