
II. Indications: Positive Pressure Ventilation
III. Contraindications: Relative (Exercise caution)
- Severe facial Trauma
- Open eye injuries
- Oral cavity with foreign body
V. Device: Flow-inflating bag (Anesthesia Bag)
- Mechanism
- Requires compressed oxygen source to fill
- Advantages
- Preferred for Newborn Resuscitation
- Lung Compliance can be felt on squeezing bag
- Can deliver free-flow 100% oxygen
- Disadvantages
- Requires a tight facial seal
- Higher risk of over-inflating lung (use manometer)
- Technically more difficult to learn to use
- Technique
- Set oxygen supply flowmeter to 5-10 L/min
- Adjust bag volume with flow-control valve
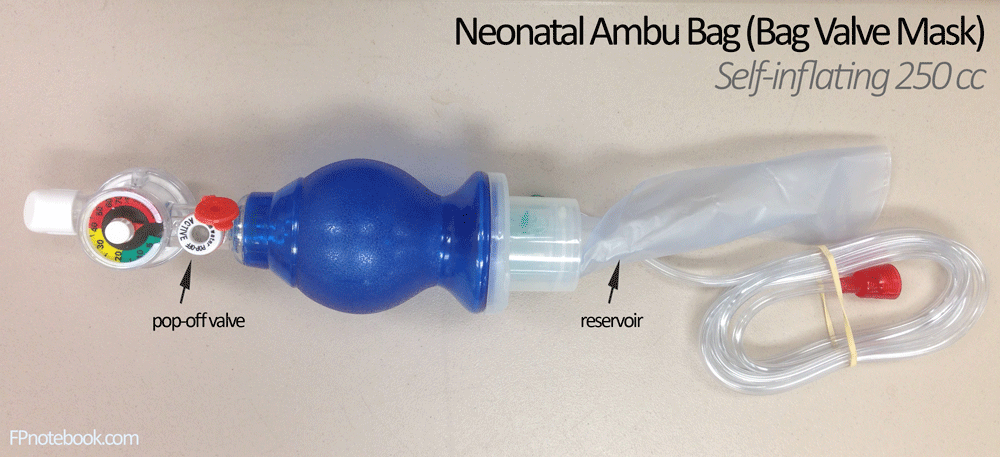
VI. Device: Self-inflating bag (Bag-valve mask or Ambu Bag)
- Aduncts (see below)
- PEEP Valve
- Impedance Threshold Device (e.g. ResQPOD)
- Mechanism
- Bag fills spontaneously after being squeezed
- Advantages
- Does not require an oxygen source
- Easier to learn to use
- Disadvantages
- Can not deliver free flow oxygen
- Place Nasal Cannula 15 lpm below mask to deliver continuous oxygen
- Delivered oxygen is diluted with room air entrained through the exhalation port
- Apply a PEEP Valve to increase Oxygen Delivery
- Can not deliver free flow oxygen
-
Oxygen Delivery with ventilation (Bag-Valve Mask)
- No Oxygen Source
- Delivers 21% Oxygen (Room air)
- Without Oxygen Reservoir
- Delivers 30-80% Oxygen at 10 LPM flow
- With Oxygen Reservoir (required for high oxygen flow)
- Delivers 60-95% Oxygen at 10-15 LPM flow
- Delivers oxygen if reservoir fills
- No Oxygen Source
- Pop-Off Valves (Bag Valve Mask)
- Usually set at 30-45 cm H2O
- Pop-off should be easily occluded on bags
- Higher pressures are needed during CPR
- Occlusion of the pop off valve
- Depress valve with finger during ventilation or
- Twist the pop-off valve into closed position
- Monitoring
- End-Tidal CO2
- Place device between bag and mask
- Confirms that delivered breaths are matched with CO2 exhalation
- Mask pressure gauge
- Available with some bag-valve masks via built-in gauge or via accessory port
- Ideally present to monitor delivered pressure with each gauge (prevents hyperinflation)
- Exercise caution, when a gauge is not present to avoid hyperinflation
- Target pressures
- Green zone: 20 mmHg (do not exceed 30 mmHg)
- End-Tidal CO2
- Images
- Neonatal Ambu-Bag
- Neonatal Ambu-Bag
VII. Device: Self-inflating Bag (Bag Valve Mask) Adjuncts
- PEEP Valves
- Put PEEP Valve on every bag-valve-mask
- PEEP Valves dramatically improve Oxygen Delivery
- One-way valve that blocks flow out of the exhalation port unless pressure exceeds set value (PEEP)
- PEEP keeps alveoli open between ventilations
- Blocks room air from entering the exhalation port (prevents dilution of supplied oxygen with room air)
- May set the PEEP Valve to 0, if only wish to raise delivered oxygen without applying PEEP
- One-way valve that blocks flow out of the exhalation port unless pressure exceeds set value (PEEP)
- Adverse Effects
- Increases risk in Hypotension of decreasing venous return (increases intrathoracic pressure)
- References
- Levitan (2013) Practical Emergency Airway Management Course
- Impedance Threshold Device (e.g. ResQPOD)
- May be indicated in CPR (but variable evidence)
- Attaches inline between positive pressure device (e.g. ambubag) and mask or ET Tube
- Assists in maintaining negative intrathoracic pressure which in turn increases venous return
- Associated with increased rate of Return of Spontaneous Circulation
- However more recent studies showed no benefit
VIII. Device: Noninvasive Positive Pressure Ventilation (NIPPV)
IX. Precautions
- Do not use Bag Valve Mask to deliver free flow oxygen
- Oxygen only flows when squeezing bag
- Use Bag Valve Mask with a PEEP Valve and Nasal Cannula at 15 lpm under mask to deliver oxygen
- Position patient for best ventilation (Oops Mnemonic, Levitan)
- Oxygen On
- Apply 15 lpm by Nasal Cannula under mask for Apneic Oxygenation
- Pull Mandible forward (Jaw Thrust maneuver)
- Sit patient up (to 20 degrees)
- Anticipate difficult mask ventilation (Mnemonic: MOANS)
- Mask seal (e.g. beard)
- Obstruction
- Older Age
- No teeth (replace dentures for Bag Valve Mask Ventilation)
- Stiff lungs requiring increased Ventilatory pressures (Asthma, COPD, ARDS, term pregnancy)
- References
- Difficult Airway Course
X. Technique
-
Tidal Volume
- Term Newborns
- Administer 5-8 ml/kg (15 to 25 ml per ventilation)
- Bag volume: 200 to 750 ml (usually >450 ml)
- Adults and older children
- Administer 6-7 ml/kg (lower than prior recommendations for 10-15 ml/kg)
- Term Newborns
- Hold mask over face with one hand
- Mask should fit snugly
- Covers mouth, nose and chin
- Should not cover eyes
- Use C-E position
- Operator forms a "C" with their first 2 fingers applying pressure to seal mask over nose and mouth
- Thumb over the mask top (nose)
- Index finger over the mask bottom (mouth)
- Operator forms an "E" with their last 3 fingers under the jaw
- Use fingers to support the jaw, pulling the face into the mask
- Operator forms a "C" with their first 2 fingers applying pressure to seal mask over nose and mouth
- Avoid submental pressure (risk of airway obstruction)
- Employ assistant when unable to obtain adequate seal with one hand
- Obese patients
- Patients with dentures (consider leaving dentures in for better mask fit)
- Facial hair
- Clinician with small hands or inadequate strength
- Mask should fit snugly
-
Head Tilt - chin lift (Avoid if Trauma!)
- Use Jaw Thrust maneuver in Trauma or suspected spine injury
- Infants/Toddlers
- Neutral sniffing position without hyperextension
- Children >2 years
- Anterior displacement of c-spine
- Folded towel under neck and head
- Observe for adequate ventilation
- Adequate chest rise
- No signs of gastric insufflation
XI. Protocol: Troubleshooting
- No chest rise:
- Reposition head
- Ensure mask is snug
- Lift the jaw
- Consider suctioning airway
- Consider equipment failure (always test before use)
- Test bag with hand occluding patient outlet
- Check for bag leak
- Check flow-control valve
- Check that oxygen line is connected
- Consider airway adjuncts
- Avoid Stomach insufflation and gastric distention
- Apply cricoid pressure (Sellick maneuver)
- In unconscious infant or child
- Consider NG suction
- Apply cricoid pressure (Sellick maneuver)
- Sudden decrease in Lung Compliance
- Right main Bronchus intubation
- Obstructed Endotracheal Tube
- Pneumothorax
XII. Resources
- Bag-Valve-Mask Demonstration Video (NEJM)
XIII. References
- Mason and Levitan in Herbert (2018) EM:Rap 18(1):14
- Swaminathan and Weingart in Herbert (2019) EM:Rap 19(7):6-7