
II. Indications: First-line Shoulder evaluation
III. Views: Standard
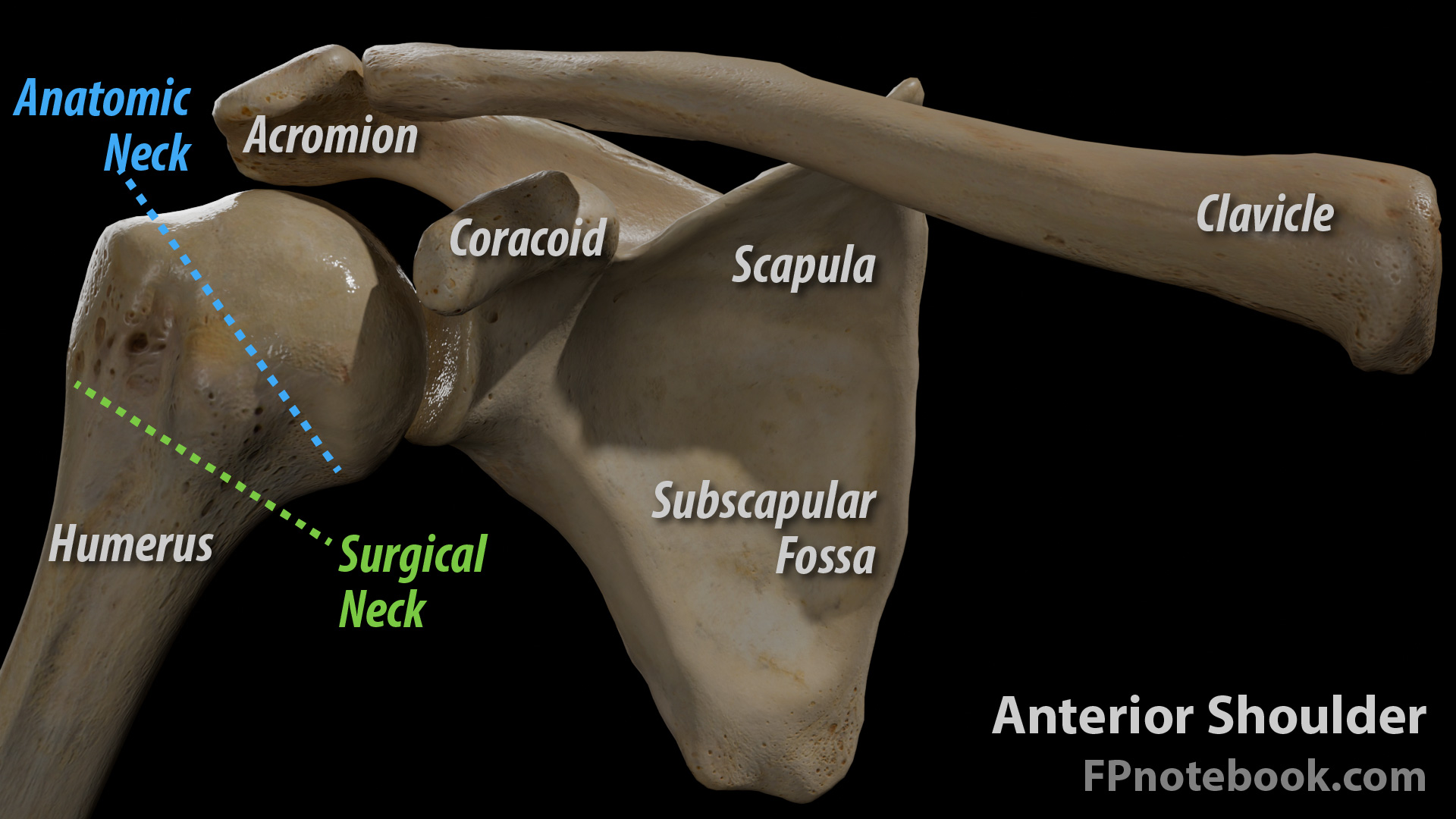
- Anterior-posterior (AP)
- Arm is typically externally rotated on a standard view
- May be internally rotated to better visualize the lesser tubercle
- May be left in neutral rotation in cases of Trauma
- Landmarks
- Humeral greater tuberosity
- AC Joint (acromion and clavicle)
- Inferior border of clavicle should align with the inferior border of acromion
- Glenohumeral Joint (glenoid, humeral head)
- Humeral head should overlap the glenoid (rim sign)
- Humeral head should appear asymmetric toward the glenoid
- Contrast with symmetric appearance in posterior dislocation (light bulb sign)
- Arm is typically externally rotated on a standard view
- Orthogonal View options
- Axillary View (preferred in Osteoarthritis, Dislocation, but requires arm manipulation)
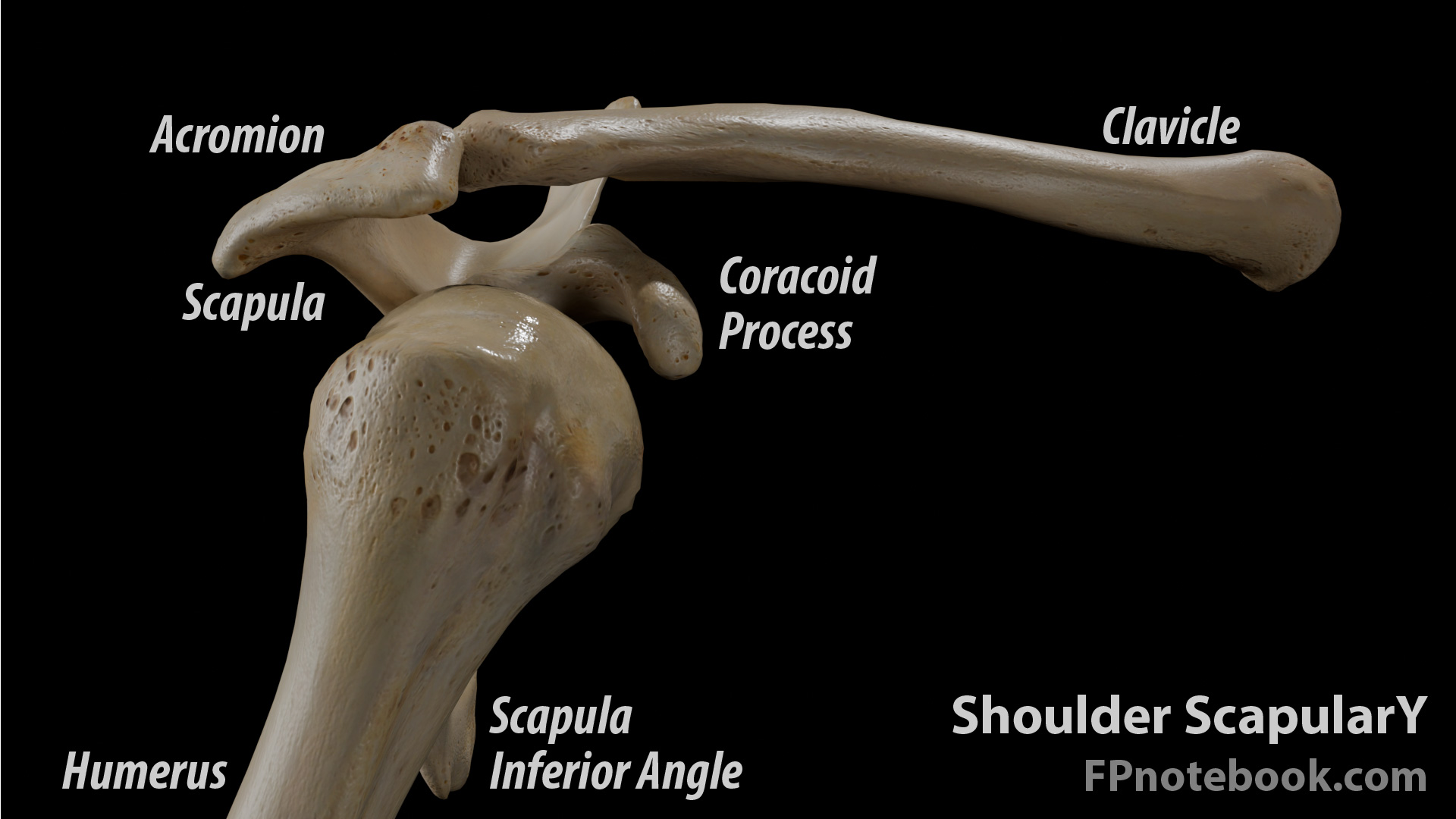
- Scapular Y View (alternative, lateral view which does not require repositioning of the arm)
- Image is perpendicular to the Scapular blade, forming a "Y" at the superior aspect
- Humeral head should be centered within the top of the Y
- Glenoid is at the center of the Y
- Images
IV. Views: Impingement Series
- Anterior-posterior
- External rotation
- Outlet Y
- West Point
V. Views: Instability Series
- Anterior-posterior with and without Rotation
- Stryker Notch
- West Point
VI. Findings: Acute Shoulder Injury
VII. Findings: Chronic Shoulder Pain
- Acromioclavicular Osteoarthritis
- Glenohumeral Osteoarthritis
- Signs of Rotator Cuff conditions
- Superior migration of humeral head (large Rotator Cuff Tear)
- Humeral head cystic changes
- Inferior acromion sclerosis
- Signs of prior Anterior Shoulder Dislocation
- Hill-Sachs Lesion (posterior humeral head indentation)
- Impact occurs when Shoulder dislocates anterior to glenoid
- Hill-Sachs Lesion (posterior humeral head indentation)
- Signs of Osteoarthritis
- Axillary view best demonstrates joint space narrowing
- Subchondral sclerosis and osteophytes may also be seen