
II. Epidemiology
- Most common elbow Fractures in Children
- Age of onset ranges between 2 and 12 years of age (peaks between 5 and 8 years of age)
- Gender: Twice as common in boys
III. Definitions
- Supracondylar Fracture of Humerus
- Distal Humerus Fracture above the epicondyles and above the Physis
IV. Pathophysiology
- Supracondylar region of the Humerus is the weakest part of the elbow (Humerus flattens, and widens)
- Mechanisms
- Direct blow to Posterior Elbow (uncommon)
- Fall on an outstretched hand with extended elbow (most common)
- Results in an extension type injury with posterior displacement of the distal Humerus (95% of cases)
V. Exam
- Vascular
- Capillary Refill
- Radial Pulse and Ulnar Pulse
- Pulse may be absent despite warm, pink hand due to collateral circulation
- Absent pulse is an indication for emergent surgical intervention
- Skin
- Open Skin Wound overlying Fracture (Open Fracture)
- Skin Tenting
- Skin puckering
- Seen with local subcutaneous Hemorrhage (e.g. brachialis Muscle penetrated by bone shard)
- Palpation
- Humeral Condyle tenderness
- Decreased elbow range of motion
- Neurologic
- Median Nerve function
- Anterior interosseous branch injury is most common
- Test with patient opposing thumb and index finger tips ("make OK sign")
- Ulnar Nerve function
- Radial Nerve function
- Median Nerve function
-
Compartment Syndrome
- Pain, Pallor, Paresthesias, Pulselessness and Poikilothermia (5 P's)
- Distal finger passive range of motion is painful
VI. Imaging
- See Elbow XRay
- Obtain a true lateral Elbow XRay
- Posterior fat pad sign
- Always abnormal
- May be only finding in a Type 1 supracondylar Fracture
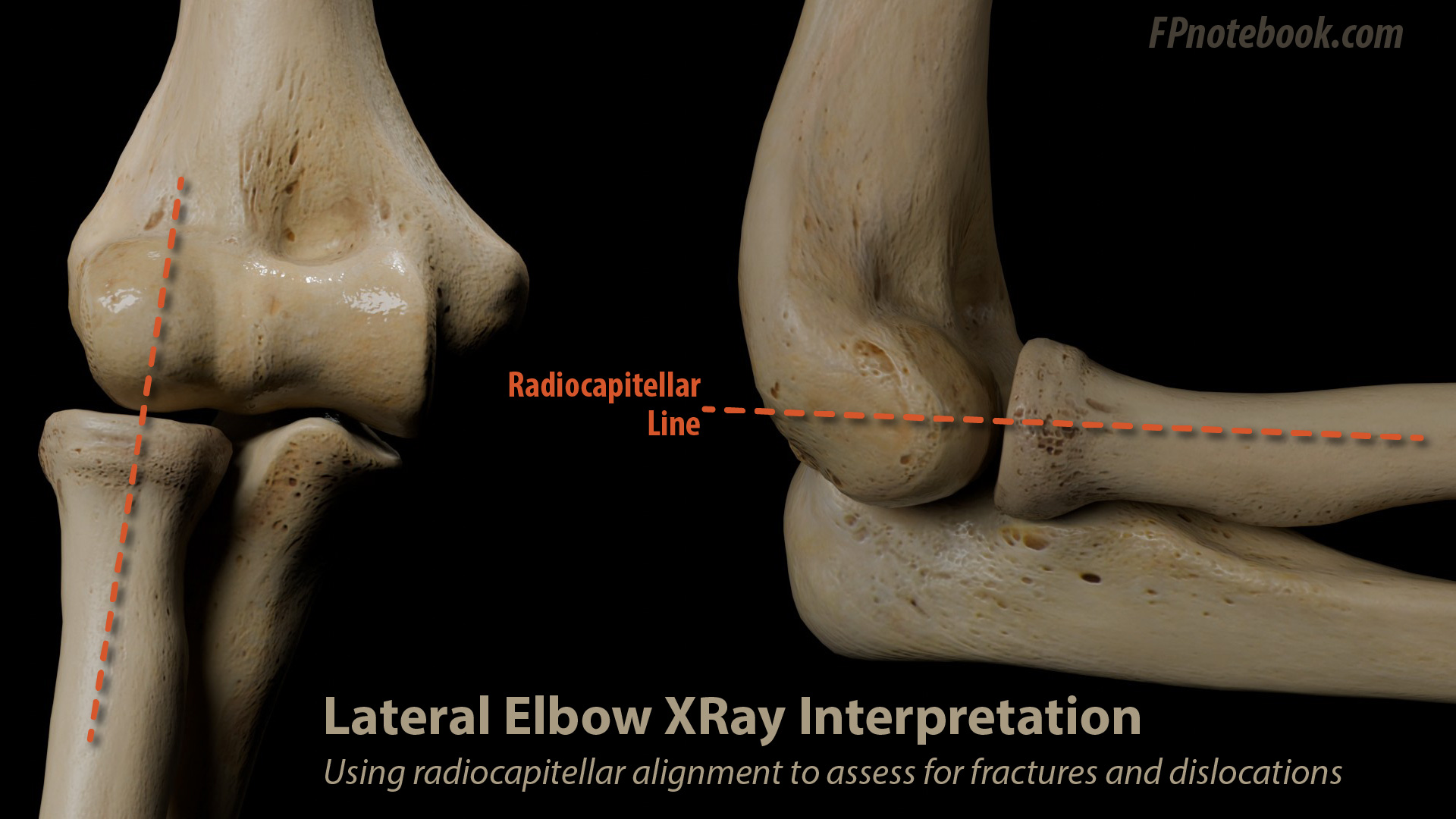
- Anterior humeral line
-
Radiocapitellar Line
-

- Line drawn down the mid proximal radius should bisect the capitellum
-
- Cortical Disruption
- See grading below (based on anterior and posterior cortical disruption)
- Extension Fracture (most common)
- Distal fragment displaced posteriorly
VII. Grading
- Type 1: Non-displaced or minimally displaced
- Type 2: Distal anterior fragment displaced and intact posterior cortex (displacement, but still partial bony apposition)
- Type 3: Displaced and no contact between Fracture fragments (both anterior cortex and posterior cortex disrupted)
VIII. Management
- Orthopedic referral in all cases
- Emergent surgical intervention for neurovascular deficit
- Urgent surgical reduction by orthopedic surgery
- Type 1 Fracture
- Splint initially
- Long Arm Splint or Double Sugar-Tong Splint with elbow in 80-90 degrees flexion
- Cast
- Splint initially
- Type 2 Fracture
- Splint as above
- Gentle flexion to 30-40 degrees is sufficient to avoid manipulating into a neurovascular injury
- Urgent orthopedic referral to determine whether Casting will be sufficient
- Open reduction and internal fixation in some cases
- Splint as above
- Type 3 Fracture (unstable Fracture)
- Splint as above for stability in gentle flexion (30-40 degrees) and emergent Consultation
- Open reduction and internal fixation in all cases
- High risk for Compartment Syndrome (controlled reduction to reduce manipulation and swelling)
IX. Complications: Type 3 Fracture
- Malunion or poor healing
- Secondary to severe displacement, incomplete reduction, or significant Soft Tissue Injury
- Gun stock deformity
- Elbow varus angulation and loss of full elbow extension
- Compartment Syndrome
- Nerve injury (transient Neuropraxia typically resolves in weeks after injury)
- Volkmann's Ischemia with contracture
- Due to local swelling and compounded by tight Splinting or cast
- Avoid excessive compression when applying splint
- Results in a combined median and Ulnar Neuropathy
- Due to local swelling and compounded by tight Splinting or cast
- Median Nerve injury
- Radial Nerve injury
- Anterior interosseus nerve injury
- Motor function only: Thumb and index finger flexion
- Volkmann's Ischemia with contracture
- Vascular injury
- Brachial artery injury (rare)
X. References
- Eiff (2012) Fracture Management for Primary Care, Saunders, Philadelphia, p. 265-6
- Wolfe and Santillanes (2021) Crit Dec Emerg Med 35(10): 12-3