
II. Pathophysiology
- Right atrial reentry circuit around the tricuspid ring
- Macro-reentry Tachycardia
- Reentry around the entire atrium
- Contrast with micro reentry circuits around smaller regions (e.g. AV Node)
III. Types
- Type I Atrial Flutter (typical)
- Constant atrial rate of 240 to 350 beats per minute
- Natural rate is altered by age, atrial dilation and Antiarrhythmics (esp. Type Ia or Type Ic)
- Ventricular rate will usually be at least a 2:1 block (or 3:1 or 4:1)
- AV Node prevents rates above 180
- Type II
- Constant atrial rate at 340 to 440 beats per minute (Faster Atrial Flutter rate than with Type I)
- Differs from Type I in reentry accessory path
IV. Signs
- Constant atrial rate
- Atrial to ventricular rates may range from 1:1 to 4:1
- Atrial to ventricular rate 2 to 1 (most common)
- Atrial rate of 240 to 350 beats per minute
- Ventricular rate 140-150 beats per minute
V. Differential Diagnosis
-
Atrial Fibrillation
- Irregular rhythm without Flutter Waves
- Patient may fluctuate between Atrial Fibrillation and Atrial Flutter on the same EKG
- Sinus Rhythm
- Flutter Wave may be difficult to identify in 2:1 block, and regular rhythm at 150 bpm may be mistaken for NSR
- Atrial Flutter is typically obvious with 3:1 or 4:1 blocks in which the Flutter Waves are easily identified
- However, sinus rhythm responds to specific management for cause (e.g. IV fluids in Dehydration)
- Atrial Flutter, in contrast will maintain a contant ventricular rate
- Flutter Wave may be difficult to identify in 2:1 block, and regular rhythm at 150 bpm may be mistaken for NSR
VI. Diagnostics: EKG
- Constant atrial rate
- Atrial rate: 300 per minute (typical)
- Atrial to ventricular rate
- Ratio 1:1 - 300 bpm (Rare, but potentially lethal)
- Ratio 2:1 - 150 bpm (most common)
- Ratio 3:1 - 100 bpm
- Ratio 4:1 - 75 bpm
- Saw tooth Flutter Waves (F Wave)
- Flutter Waves are best seen in the inferior leads
- May be difficult to visualize at a 2:1 AV Block (rate 140-150) due to overlapping QRS Complex with Flutter Wave
- Increase EKG "paper speed" to 50 mm/sec (rapid) to spread out complexes (P Waves may be seen)
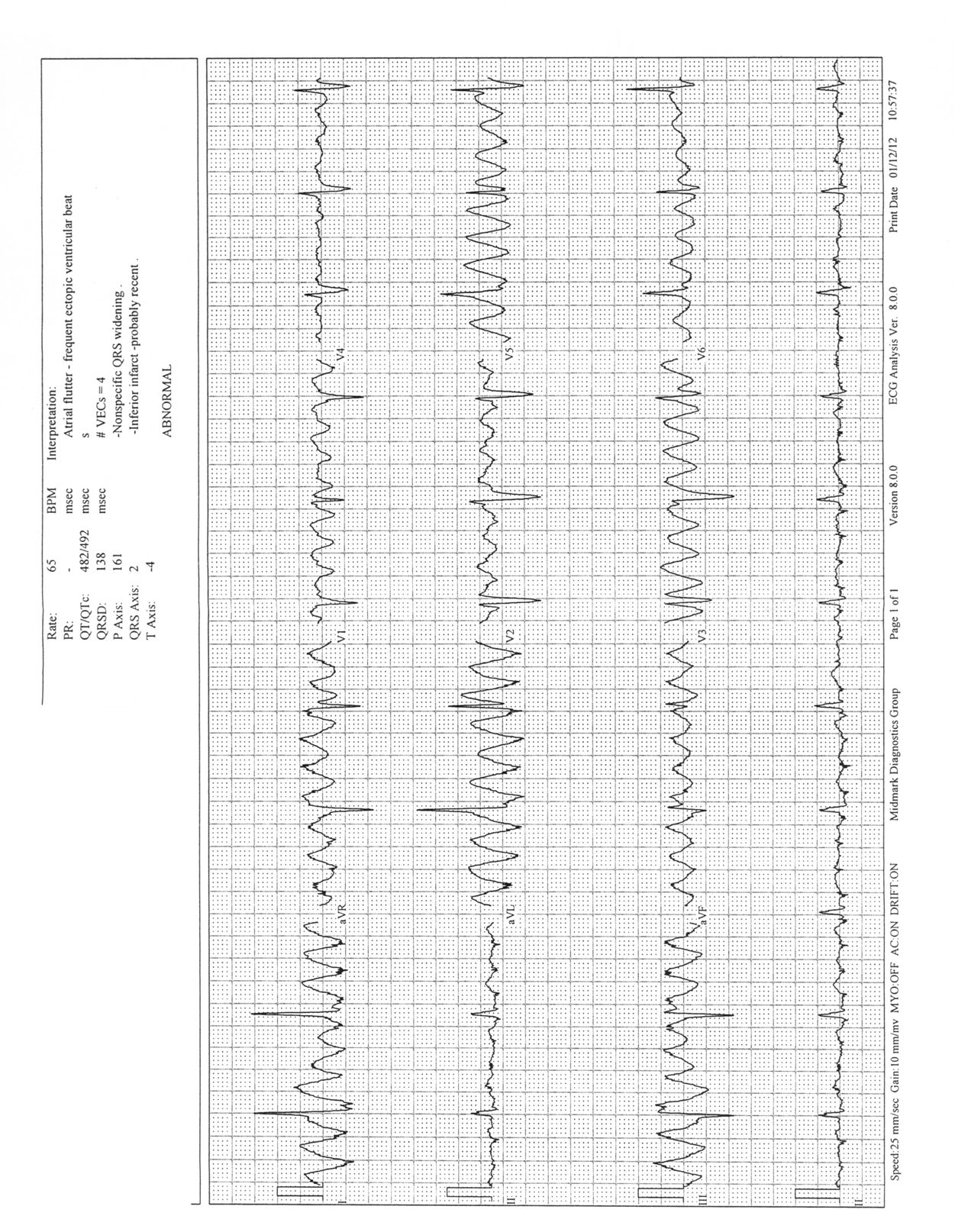
- Images
VII. Management
- See Atrial Fibrillation Management
- Highly responsive to Synchronized Cardioversion at low energy levels
- Dr. Amal Mattu (paraphrased): "you could rub your shoes on the carpet to shock Atrial Flutter back to sinus"
- However Atrial Flutter is often resistant to rate control agents (Metoprolol, Diltiazem)
VIII. References
- Berberian (2023) Crit Dec Emerg Med 37(3): 14-5