
II. Indications
IV. Safety
- Safe during pregnancy, postpartum and in Lactation
V. Preparation
- Needle: 27 gauge (1.5 inch)
-
Corticosteroid
- Methylprednisolone: 20-40 mg or
- Celestone Soluspan: 1 ml
- Triamcinolone 20-40 mg or
-
Anesthetic
- Lidocaine 1%: 2 ml or
- Bupivacaine (Marcaine) 0.25% 2 ml
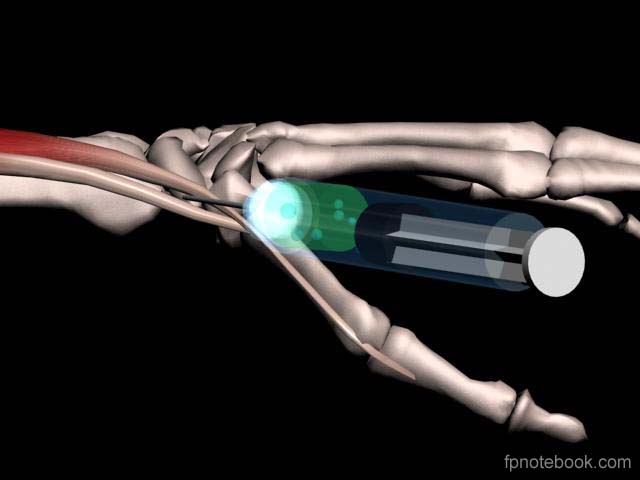
VI. Technique
- Images
-
Wrist and hand position
- Maximally abduct thumb (accentuates abductor tendon)
- Injection site
- Snuffbox at base of thumb
- Between two tendons in dorsal wrist compartment 1
- Abductor pollicis longus
- Extensor pollicis brevis
- Needle insertion
- Apply antiseptic to skin (e.g. Betadine)
- Aim 30-45 degrees proximally toward radial styloid
- Insert needle between the 2 tendons (not in tendon)
- Do not inject if Paresthesias (see below)
- Warning
- Do not inject directly into tendon
- Distal Paresthesias with needle before steroid
- Indicates needle at sensory branch of Radial Nerve
- Do not inject here!
- Withdraw and redirect needle 2-3 mm to either side
VII. Follow-up
- Consider Splinting after injection
- May be repeated up to 1-2 times at 7-14 day intervals
VIII. References
- Greene (2001) Musculoskeletal Care, p. 234
- Neustadt in Roberts (1998) Procedures, p. 914-5
- Pfenninger (1994) Procedures, Mosby, p. 1036-54
- Tallia (2003) Am Fam Physician 67(4):745-50 [PubMed]