
II. Pathophysiology
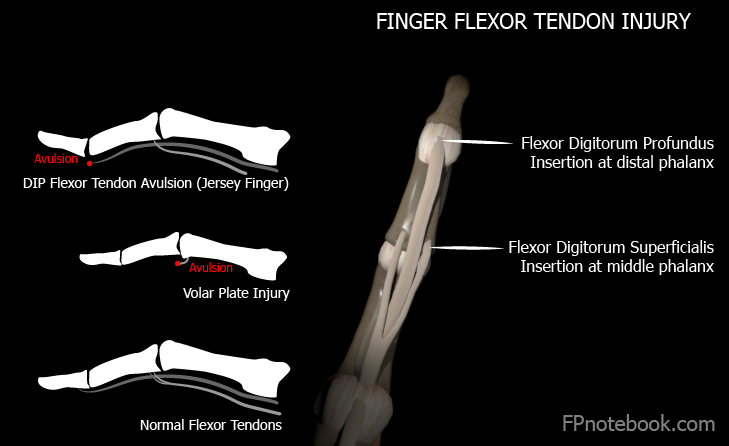
- Avulsion of the flexor digitorum profundis tendon
- Images
III. Mechanism
- Ring finger most commonly affected (75% of cases)
- Protrudes further than other fingers on grasping
- Forced hyperextension of an actively flexed DIP joint
- Results in avulsion Fracture at the bony insertion (on distal phalanx) of the flexor digitorum profundus tendon
- Example
- Football player grabs a player's jersey on tackle
- Lifting latch on car door
IV. Symptoms
- Pain and swelling at volar aspect of DIP
- Localized tenderness and fullness if tendon retraction
- Affected finger more extended at DIP when hand at rest
- Inability to flex at affected DIP joint
V. Signs
- Do not passively force finger into extension
- Avulsed tendon retracts with avascular risk
- Assess Profundus
- Hold proximal interphalangeal joint (PIP)
- Test active flexion of distal Interphalangeal joint
- Avulsion results in inability to flex at DIP
- FDP Tendon may retract to the palm
- Assess for flexor digitorum superficialis rupture
- Hold all fingers except affected finger in extension
- Test proximal interphalangeal joint (PIP) flexion
VI. Imaging: XRay digit (AP, Lateral, Oblique)
- Assess for bony avulsion of volar distal phalanx
VII. Management
- Early surgical repair in all cases
- Temporize by Splinting finger in current position
- PIP and DIP joints in slight flexion
- Hand surgeon or orthopedics referral
- Best recovery if repaired within 7-10 days of injury
- Post-Operative Management
- No sports participation until fully recovered
- Hand therapy during recovery period
- Expect recovery over 6 to 12 weeks
VIII. Complications
- Fibrosis and scarring of tendon sheath
- Flexor digitorum profundus contracture with flexion deformity
- Associated with delayed surgical repair
IX. References
- Brandenburg (1996) Consultant p.331-340
- Calmbach (1996) Lecture in Minneapolis
- Dvorak (1996) Lecture in Minneapolis
- Lillegard (1996) Lecture in Minneapolis
- Childress (2022) Am Fam Physician 105(6): 631-9 [PubMed]
- Wang (2001) Am Fam Physician 63(10):1961-66 [PubMed]