
II. Advantages
- Ischemic EKG changes best acute MI evidence
- Applies if symptom onset within last 3 hours
- Normal/Nondiagnostic initial EKG predicts low risk
III. Disadvantages
- Poor sensitivity for Myocardial Infarction (40-50%)
- 3-10% of MI patients have initial normal EKG
- 25% of patients with missed MI had misread EKG
IV. Precautions
- The computer over-reads abnormal EKGs
- Compare with prior EKGs (Increases Test Specificity)!
- Obtain serial EKGs if initial EKG is non-diagnostic
- May repeat EKG every 15 min for 1-2 hours
- Consider Myocardial Ischemia if ST depression >0.5 mm
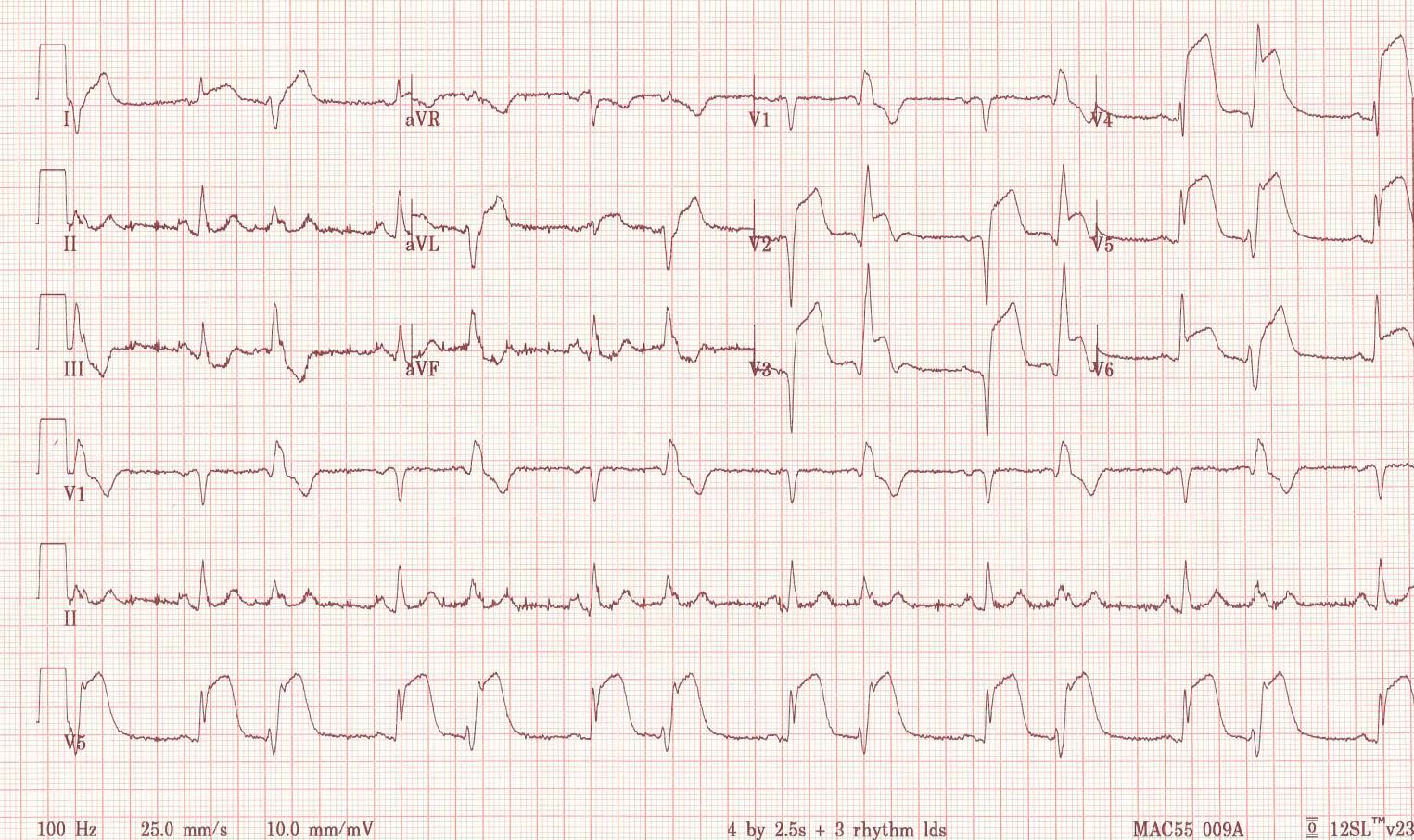
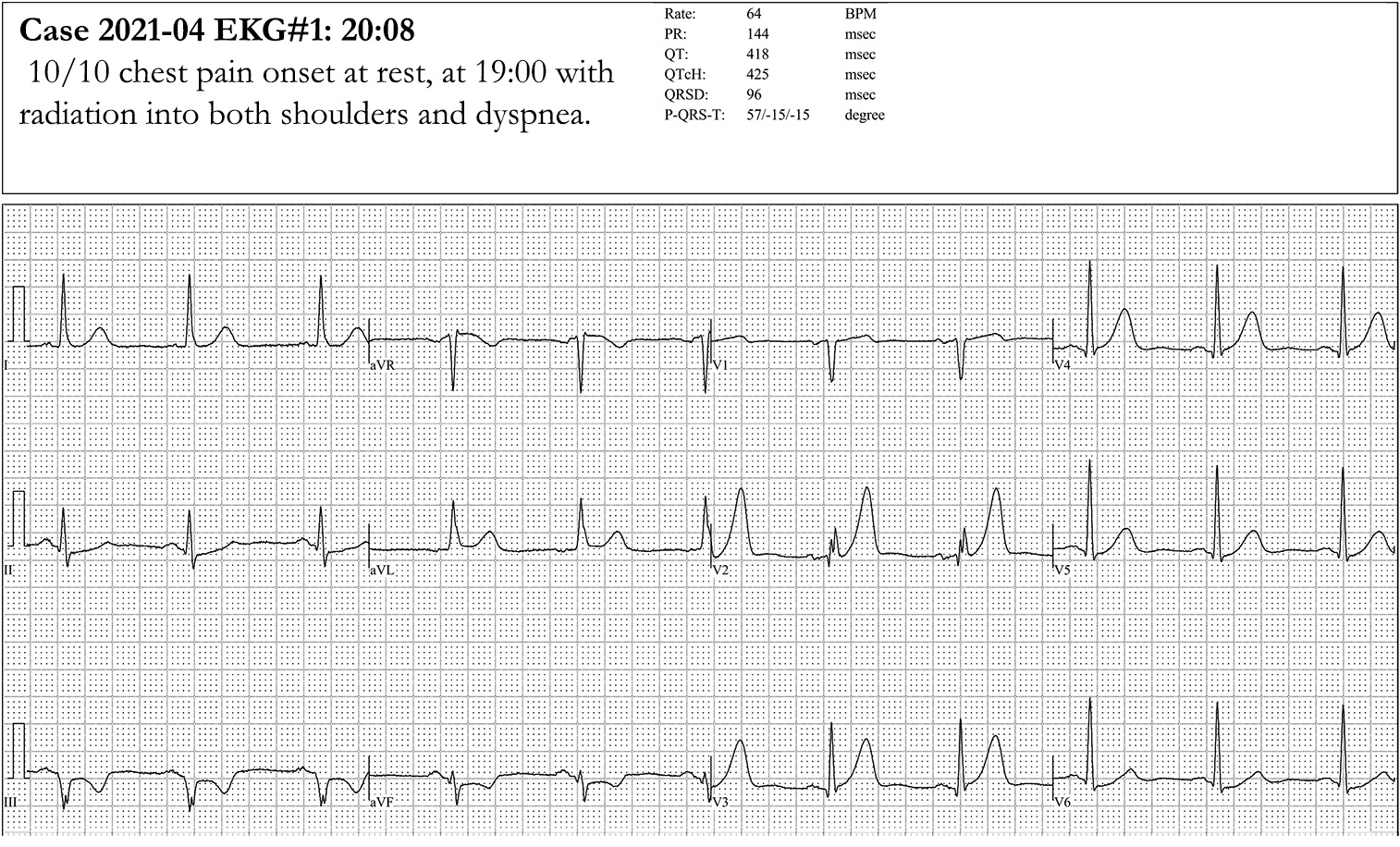
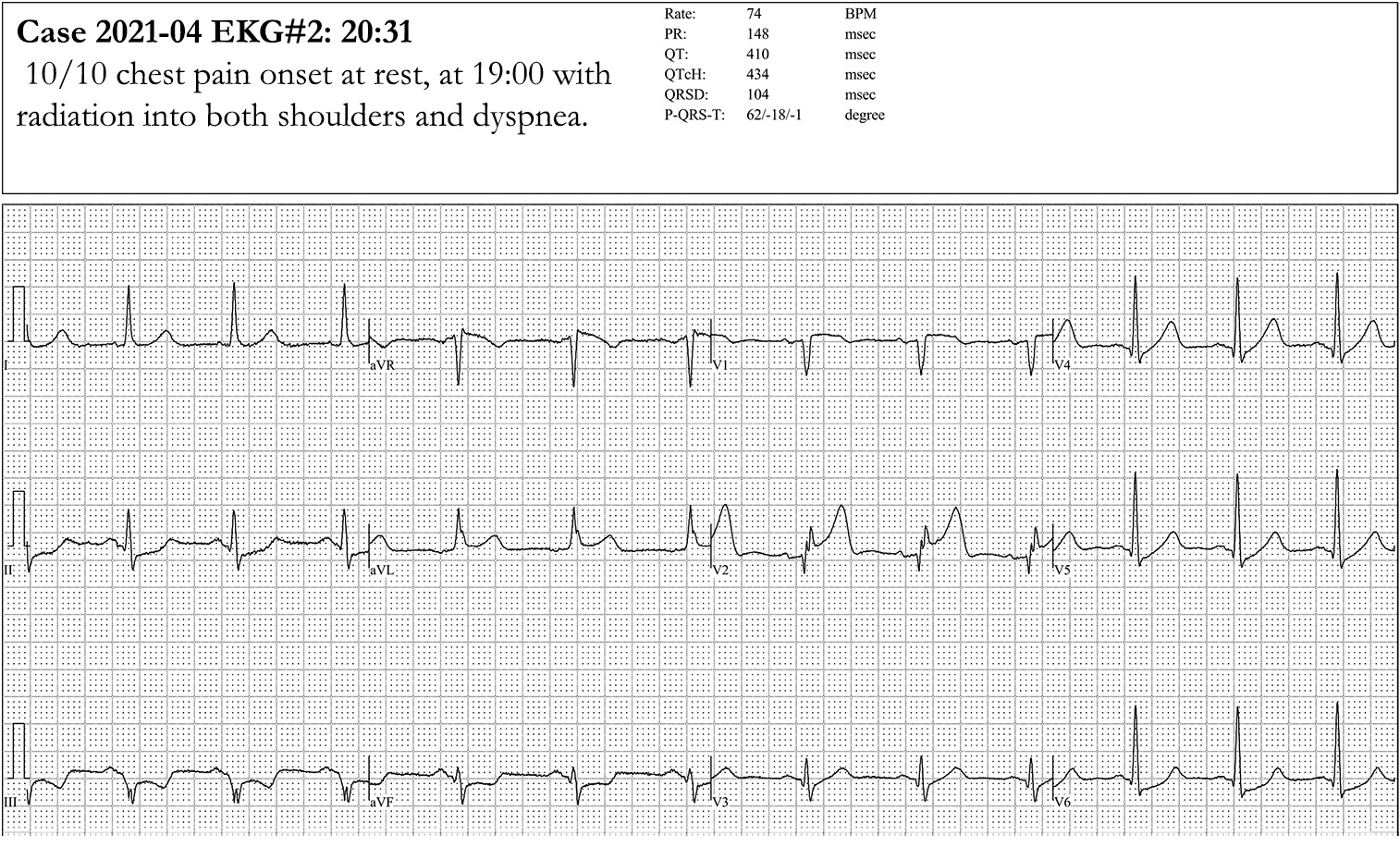
V. Images
- Acute ST Elevation Myocardial Infarction with delayed presentation (ST Elevation and Q Waves present)
- Acute ST Elevation Myocardial Infarction evolving from Hyperacute T Waves
VI. Findings: EKG Markers of underlying CAD
- Left Ventricular Hypertrophy
- ST Segment changes
- T Wave changes
- Diagnostic Q Waves in 2 contiguous leads
- Left Bundle Branch Block or other conduction changes
VII. Findings: General EKG Changes suggestive of Myocardial Ischemia
- Electrocardiogram may be completely normal
-
ST Elevation or ST depression
- Over 1 mm ST changes that are transient with symptoms
- Summed ST deviation (sum of affected leads) >2.5 mm
- ST Elevation criteria in leads V2-V3 varies by age and gender
- Men age <40 years old
- V2-V3 ST Elevation >2.5 mm
- Accounts for Early Repolarization in young men
- Men age >40 years old
- V2-V3 ST Elevation >2 mm
- Women
- V2-V3 ST Elevation >1.5 mm
- Men age <40 years old
- Deep symmetric T-wave inversion
- Occurs in multiple precordial leads
- Left main Coronary Artery stenosis marker
- ST Depression >1 mm in 8 or more leads (esp I, II, V4-6) AND ST Elevation in aVR, aVL or V1
- Suggests multi-vessel ischemia or left main obstruction
- aVR ST Segment Elevation > V1 ST Segment Elevation
- Biphasic or Deep T Wave Inversion in V2, V3 (Wellen's Syndrome)
- High risk for left anterior descending artery ischemia and Anterior Wall Myocardial Infarction
- ST Depression >1 mm in 8 or more leads (esp I, II, V4-6) AND ST Elevation in aVR, aVL or V1
- Left Anterior Descending Artery Occlusion
- Hyperacute T Waves with J Point Depression (De Winter T Waves, seen in 2% of LAD lesions)
- J Point depression with upsloping ST Segment AND
- Tall, prominent, hyperacute precordial T Waves
- Hyperacute T Waves also seen in Hyperkalemia, STEMI without J Point depression
- Hyperacute T Waves with J Point Depression (De Winter T Waves, seen in 2% of LAD lesions)
VIII. Findings: General EKG Changes suggestive of Acute Myocardial Infarction
- New left ventricular strain pattern
-
New Left Bundle Branch Block
- Sgarbossa Criteria and Modified Sgarbossa Criteria may identify STEMI despite Left Bundle Branch Block (or right ventricular Pacemaker)
-
Q Waves
- At least 0.04 sec wide and 1/3 height of R Wave
- Unless isolated in Lead III
-
T Wave Inversion
- Significant unless isolated to Lead III or Lead V1
- T Wave must be at least 1 mm deep
- T Wave Inversion within 4 hours of reperfusion is a reassuring prognostic sign
- ST-T elevation (>1mm in limb or precordial leads)
- Must have >=2 concordant leads with changes
- ST depression in Lead V1, Lead V2 (Posterior MI)
-
Hyperacute T Waves (over 50% of preceding R)
- Must have 2 or more leads with changes
IX. Findings: Septal MI Anatomic Distribution
-
Electrocardiogram Changes
- Lead V1 to lead V2
- Distribution
- Left Coronary Artery: LAD-Septal Branch
- Complications
- Infranodal and Bundle Branch Block
X. Findings: Anterior MI Anatomic Distribution
- EKG Changes
- ST Elevation in lead V2 to lead V4
- ST depression in leads II, III, avF (variably present)
- Distribution
- Left Coronary Artery: LAD-Diagonal branch
- Complications
- Worse prognosis
- High risk of sudden death
- High risk of Congestive Heart Failure in first year
- Complete Heart Block
XI. Findings: Inferior MI Anatomic Distribution
- EKG Changes
- ST Elevation in leads II, III, aVF
- Q Waves in leads III, aVF
- ST depression and T Wave Inversion in lead aVL (reciprocal change)
- Distribution
- Right Coronary Artery: Posterior descending branch
- Complications
- Right Ventricular Infarction
- Inferior heart wall lies along the diaphragm
- Distended neck veins with clear lungs
- Systolic Blood Pressure drops with
- Right Ventricular Infarction
XII. Findings: Lateral MI Anatomic Distribution
- EKG Changes
- ST Segment Elevation in leads V5, V6, I, aVL
- I and aVL are considered contiguous leads (high lateral wall)
- ST Elevation in both I and aVL is considered STEMI criteria for immediate reperfusion
- ST segment Depression in leads V1, V2, V3, III, aVF (reciprocal change)
- ST Segment Elevation in leads V5, V6, I, aVL
- Distribution
- Left Coronary Artery: Circumflex branch
- Complications
- Left Ventricular Dysfunction
- AV nodal block
XIII. Findings: Right Ventricular Infarction Anatomic Distribution
- Standard EKG Changes (similar to anterior MI EKG when rotated 180 degrees)
- ST Elevation in leads I and aVF, and lead III more than II
- ST depression in leads I, aVL (reciprocal to posterior changes)
- Right sided EKG
- Right Lead Positioning
- Alternative: V4R
- Simply move V4 lead to the right chest (5th intercostal space, mid-clavicular line)
- Findings
- ST Elevation >1mm in V4R
- Q Waves are normal in right-sided leads and are not indicative of Myocardial Infarction history
- Distribution
- Right Coronary Artery: Proximal branches
- Complications
- Severe and refractory Hypotension in response to nitrates
- Treated with fluid bolus and nitrates are contraindicated
- Severe and refractory Hypotension in response to nitrates
XIV. Findings: Posterior Infarction Anatomic Distribution
- Standard EKG Changes
- ST depression in leads V1 to V4
- Differentiate from reciprocal changes in inferior-lateral MI
- Contrast with right sided infarct with ST Elevation in V1 to V4
- Tall R Wave (>0.04 seconds) in leads V1 and V2
- Interpret V2 by rotating the axis 180 degrees (or apply posterior leads)
- Tall R Wave rotates to a Q Waves
- ST depression rotates to ST Elevation
- T Wave rotates to T Wave Inversion
- ST depression in leads V1 to V4
- Posterior EKG Changes
- Leads V8 and V9 (placed on left back, below left Scapula) demonstrate ST Elevation
- ST Elevation in V8 and V9 posterior leads may be significant at 0.5 mm
- Distribution
- Distal Right Coronary Artery: Posterior descending
- Left Coronary Artery: Circumflex
- Complications